The Tow Truck Receipt form serves as a crucial document in the towing industry, capturing essential details about the towing service provided. This form includes key information such as the date and time of the tow, the identification of the tow truck, and the names and contact details of both the towing company and the customer. It also specifies the locations where the vehicle was picked up and delivered, ensuring clarity in the transaction. The receipt outlines the fees associated with the towing service, including public and private towing rates, as well as daily storage fees. Additional charges may be noted, providing transparency for both parties. Importantly, the form requires signatures from the tow truck operator and the owner of the disabled vehicle, solidifying the agreement. Finally, it reminds the towing company to retain a copy for three years, highlighting the importance of record-keeping in this line of work. Overall, the Tow Truck Receipt form is more than just a piece of paper; it is a vital tool that protects the rights of customers while ensuring that towing companies operate fairly and transparently.

Tow Control No. ____________________ |
DATE: ____________ |
Tow Crane No. _____________________ |
TIME: ____________ |
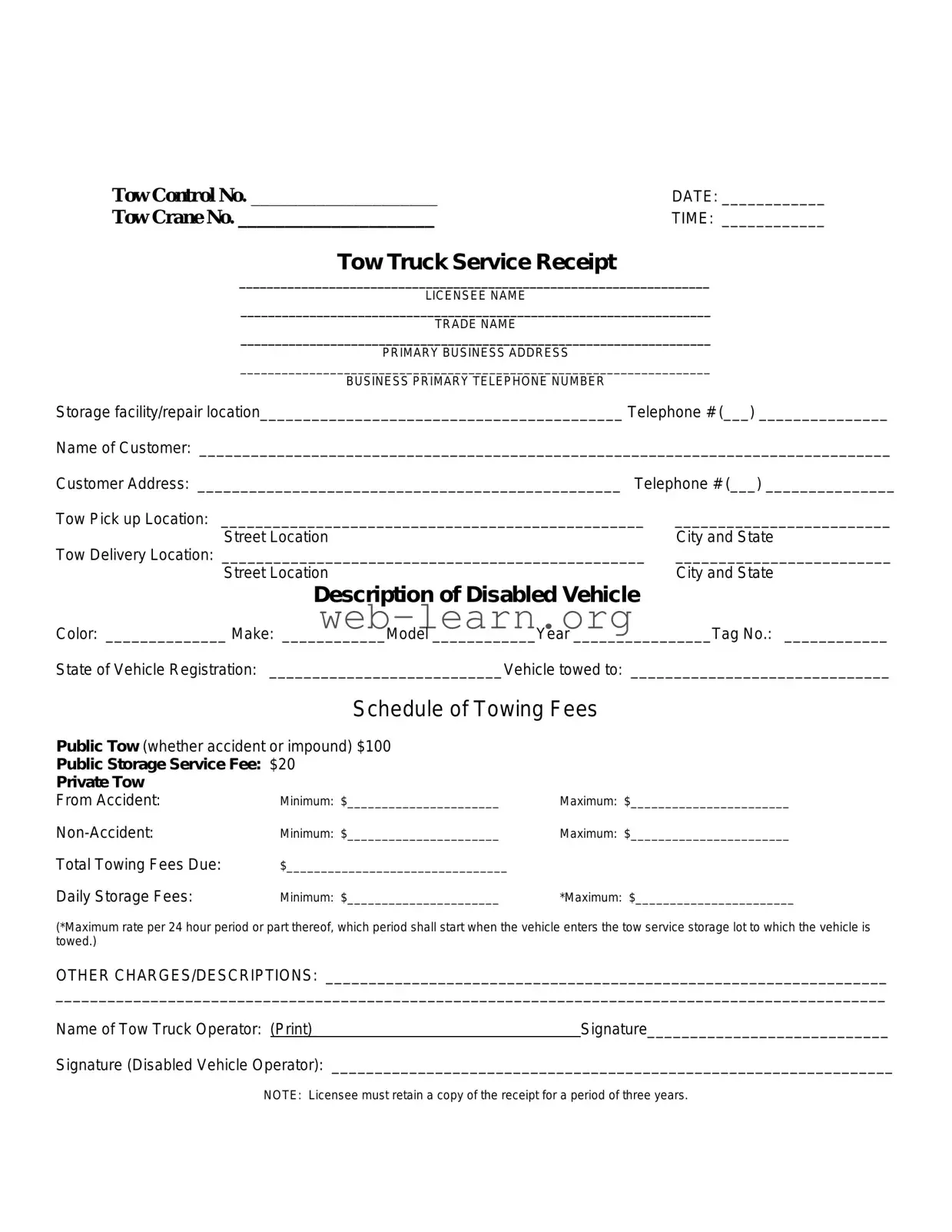
Tow Truck Service Receipt
____________________________________________________________________
LICENSEE NAME
____________________________________________________________________
TRADE NAME
____________________________________________________________________
PRIMARY BUSINESS ADDRESS
____________________________________________________________________
BUSINESS PRIMARY TELEPHONE NUMBER
Storage facility/repair location__________________________________________ Telephone # (___) _______________
Name of Customer: ________________________________________________________________________________
Customer Address: _________________________________________________ Telephone # (___) _______________
Tow Pick up Location: _________________________________________________ |
_________________________ |
Street Location |
City and State |
Tow Delivery Location: _________________________________________________ |
_________________________ |
Street Location |
City and State |
Description of Disabled Vehicle |
|
Color: ______________ Make: ____________Model ____________Year ________________Tag No.: ____________
State of Vehicle Registration: ___________________________Vehicle towed to: ______________________________
Schedule of Towing Fees
Public Tow (whether accident or impound) $100
Public Storage Service Fee: $20
Private Tow
From Accident:
Total Towing Fees Due:
Maximum: $_______________________
Maximum: $_______________________
Daily Storage Fees:Minimum: $______________________ *Maximum: $_______________________
(*Maximum rate per 24 hour period or part thereof, which period shall start when the vehicle enters the tow service storage lot to which the vehicle is towed.)
OTHER CHARGES/DESCRIPTIONS: _________________________________________________________________
________________________________________________________________________________________________
Name of Tow Truck Operator: (Print)Signature____________________________
Signature (Disabled Vehicle Operator): _________________________________________________________________
NOTE: Licensee must retain a copy of the receipt for a period of three years.
| Fact Name | Description |
|---|---|
| Minimum Charges | The receipt must indicate a minimum charge for towing services, which varies by location. |
| Tow Control Number | A unique Tow Control Number is assigned to each tow for tracking purposes. |
| Date and Time | The date and time of the tow must be recorded on the receipt to establish a timeline of events. |
| Licensee Information | Details such as the licensee's name, trade name, and business address must be included. |
| Customer Details | The receipt requires the name, address, and telephone number of the customer involved in the tow. |
| Vehicle Information | Specifics about the disabled vehicle, including color, make, model, year, and registration state, must be documented. |
| Towing Fees | A schedule of towing fees must be clearly outlined, including public and private tow rates. |
| Daily Storage Fees | Daily storage fees must be listed, specifying minimum and maximum rates applicable per 24-hour period. |
| Retention Requirement | The licensee is required to retain a copy of the receipt for a minimum of three years. |
Filling out the Tow Truck Receipt form is an important task that helps document the towing service provided. Once the form is completed, it will serve as a record for both the towing company and the customer. Follow these steps to ensure that all necessary information is accurately captured.
Once all sections are completed, keep a copy for your records as required. This ensures compliance with retention policies and provides proof of service for both parties involved.
What is the purpose of the Tow Truck Receipt form?
The Tow Truck Receipt form serves as a record of the towing services provided. It includes essential information such as the date, time, locations, vehicle details, and fees charged. This document is crucial for both the towing company and the customer, ensuring transparency and accountability in the towing process.
What information is required on the receipt?
The receipt must include:
How are towing fees determined?
Towing fees can vary based on several factors, including the type of tow (public or private), whether it was due to an accident or a non-accident situation, and any additional services required. The form outlines a schedule of fees, including a minimum charge for public tows and storage fees.
What should I do if I disagree with the charges on the receipt?
If there is a disagreement regarding the charges, it is advisable to contact the towing company directly. Discuss your concerns and provide any relevant information. If the issue remains unresolved, you may want to consider filing a complaint with local authorities or seeking legal advice.
How long should the towing company keep the receipt?
The towing company is required to retain a copy of the receipt for a period of three years. This retention is important for record-keeping and may be necessary for any future disputes or inquiries regarding the tow.
What happens if my vehicle is not claimed?
If a vehicle is not claimed within the specified time frame, the towing company may have the right to charge daily storage fees. Ultimately, unclaimed vehicles may be subject to auction or disposal, depending on local laws and regulations.
Can I request additional services during the towing process?
Yes, customers can request additional services, such as roadside assistance or storage options. However, these services may incur extra charges, which should be clearly outlined on the receipt.
Is the receipt valid for insurance claims?
Yes, the Tow Truck Receipt can be used as documentation for insurance claims. It provides proof of the towing service, details of the vehicle, and the associated costs, which may be necessary for reimbursement from your insurance provider.
Filling out the Tow Truck Receipt form accurately is crucial for both the service provider and the customer. However, several common mistakes can lead to confusion or disputes later on. Understanding these pitfalls can help ensure that the receipt is completed correctly.
One frequent error is neglecting to fill in the minimum and maximum charges. These fields are essential for establishing the financial terms of the towing service. If these amounts are left blank, it can lead to misunderstandings about how much the customer owes. Always double-check that these figures are clearly entered.
Another mistake involves omitting important identification details. The licensee name and trade name should be filled out completely. Missing this information can create issues if the customer needs to contact the towing company later. Make sure to write these names clearly to avoid any confusion.
Providing incomplete or inaccurate vehicle information is also a common mistake. The section that asks for the description of the disabled vehicle must be filled out with care. This includes the color, make, model, year, and tag number. If any of these details are incorrect or missing, it could complicate the retrieval of the vehicle later on.
Failing to include the tow control number and the date and time of the tow is another oversight that can lead to problems. These details are critical for record-keeping and can help clarify when the service was provided. Be sure to enter this information accurately to maintain a reliable record.
Many people forget to fill out the customer information section completely. This includes the customer's name, address, and telephone number. Incomplete information can hinder communication and create challenges if follow-up is necessary. Ensure that this section is fully completed to facilitate future interactions.
Another common mistake is not including the storage facility or repair location. This information is essential for both the customer and the towing company to know where the vehicle is being held. Omitting this can lead to confusion and frustration for the customer trying to locate their vehicle.
Finally, not retaining a copy of the receipt can be a significant oversight. The note at the bottom states that the licensee must keep a copy for three years. This is important for both legal and financial reasons. Keeping a copy ensures that both parties have a record of the transaction, which can be crucial if any disputes arise.
By being aware of these common mistakes and taking the time to fill out the Tow Truck Receipt form carefully, both service providers and customers can avoid unnecessary complications and ensure a smoother towing experience.
The Tow Truck Receipt form is an essential document that records the details of a towing service transaction. However, several other forms and documents often accompany it to ensure a comprehensive understanding of the service provided and to protect the rights of all parties involved. Here are five commonly used forms in conjunction with the Tow Truck Receipt:
These documents collectively enhance the transparency and accountability of towing services. They help ensure that all parties are informed of their rights and responsibilities, fostering a smoother resolution to any issues that may arise during the towing process.
When filling out the Tow Truck Receipt form, consider the following guidelines:
Understanding the Tow Truck Receipt form is essential for both service providers and customers. However, several misconceptions exist about this document. Below are five common misunderstandings:
By clarifying these misconceptions, both service providers and customers can navigate the towing process more effectively and avoid potential misunderstandings.
When filling out and using the Tow Truck Receipt form, there are several key points to keep in mind to ensure clarity and compliance. Here are some important takeaways:
By following these guidelines, you can ensure that the Tow Truck Receipt form is filled out correctly and serves its intended purpose effectively.