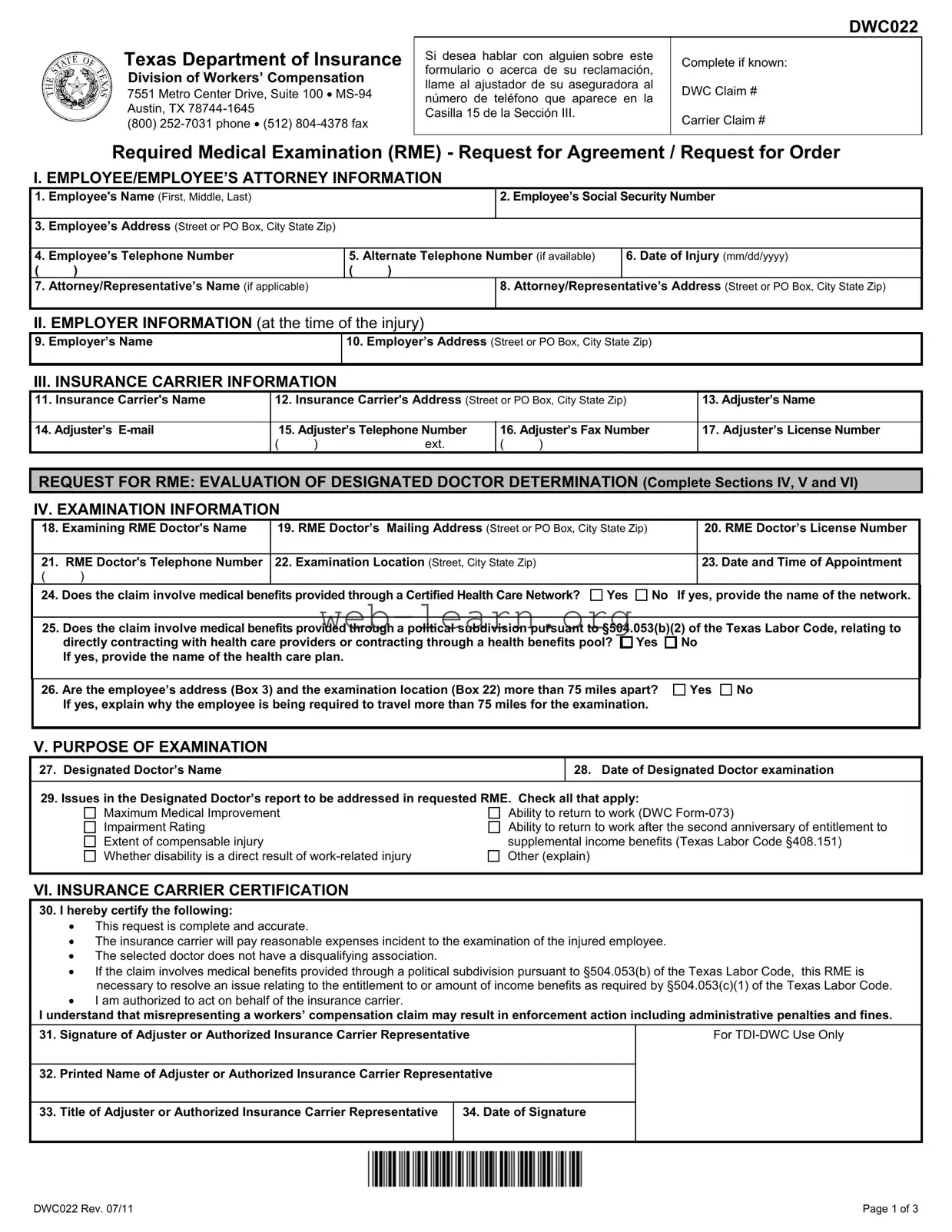
The Texas DWC022 form plays a crucial role in the workers' compensation process, specifically concerning Required Medical Examinations (RMEs). This form is utilized by insurance carriers to request an examination of an injured employee by a doctor of their choice. It serves two primary purposes: to evaluate the determinations made by a Designated Doctor and to assess the appropriateness of the health care received by the injured employee. Key information required on the form includes details about the employee, employer, and insurance carrier, as well as specifics regarding the examination, such as the doctor's name and appointment time. The form also includes sections for both the insurance carrier and the injured employee to certify their agreement or disagreement with the examination request. Understanding the nuances of the DWC022 is essential for both employees and insurance representatives, as compliance with the requirements outlined can significantly impact the outcome of a workers' compensation claim.

Texas Department of Insurance
Division of Workers’ Compensation
7551 Metro Center Drive, Suite 100 •
(800)
DWC022
Si desea hablar con alguien sobre este |
Complete if known: |
|
formulario o acerca de su reclamación, |
||
|
||
llame al ajustador de su aseguradora al |
DWC Claim # |
|
número de teléfono que aparece en la |
||
|
||
Casilla 15 de la Sección III. |
Carrier Claim # |
|
|
||
|
|
Required Medical Examination (RME) - Request for Agreement / Request for Order
I. EMPLOYEE/EMPLOYEE’S ATTORNEY INFORMATION
1. |
Employee's Name (First, Middle, Last) |
|
|
2. Employee’s Social Security Number |
|
|
|
|
|
|
|
3. |
Employee’s Address (Street or PO Box, City State Zip) |
|
|
|
|
|
|
|
|
||
4. |
Employee’s Telephone Number |
5. Alternate Telephone Number (if available) |
6. Date of Injury (mm/dd/yyyy) |
||
( |
) |
( |
) |
|
|
7. Attorney/Representative’s Name (if applicable) |
|
|
8. Attorney/Representative’s Address (Street or PO Box, City State Zip) |
||
|
|
|
|
|
|
II. EMPLOYER INFORMATION (at the time of the injury)
9. Employer’s Name |
10. Employer’s Address (Street or PO Box, City State Zip) |
|
|
III. INSURANCE CARRIER INFORMATION
11. Insurance Carrier's Name |
12. Insurance Carrier's Address (Street or PO Box, City State Zip) |
13. Adjuster’s Name |
||||
|
|
|
|
|||
14. Adjuster’s |
15. Adjuster’s Telephone Number |
16. Adjuster’s Fax Number |
17. Adjuster’s License Number |
|||
|
( |
) |
ext. |
( |
) |
|
REQUEST FOR RME: EVALUATION OF DESIGNATED DOCTOR DETERMINATION (Complete Sections IV, V and VI)
IV. EXAMINATION INFORMATION
18. Examining RME Doctor's Name |
19. RME Doctor’s Mailing Address (Street or PO Box, City State Zip) |
20. RME Doctor’s License Number |
|
|
|
|
|
21. RME Doctor's Telephone Number |
22. Examination Location (Street, City State Zip) |
23. Date and Time of Appointment |
|
( |
) |
|
|
24. Does the claim involve medical benefits provided through a Certified Health Care Network?
Yes
No If yes, provide the name of the network.
25.Does the claim involve medical benefits provided through a political subdivision pursuant to §504.053(b)(2) of the Texas Labor Code, relating to directly contracting with health care providers or contracting through a health benefits pool? Yes No
If yes, provide the name of the health care plan.
26.Are the employee’s address (Box 3) and the examination location (Box 22) more than 75 miles apart? If yes, explain why the employee is being required to travel more than 75 miles for the examination.
Yes
No
V. PURPOSE OF EXAMINATION
27. Designated Doctor’s Name
28. Date of Designated Doctor examination
29. Issues in the Designated Doctor’s report to be addressed in requested RME. Check all that apply:
Maximum Medical Improvement |
Ability to return to work (DWC |
Impairment Rating |
Ability to return to work after the second anniversary of entitlement to |
Extent of compensable injury |
supplemental income benefits (Texas Labor Code §408.151) |
Whether disability is a direct result of |
Other (explain) |
VI. INSURANCE CARRIER CERTIFICATION
30.I hereby certify the following:
•This request is complete and accurate.
•The insurance carrier will pay reasonable expenses incident to the examination of the injured employee.
•The selected doctor does not have a disqualifying association.
•If the claim involves medical benefits provided through a political subdivision pursuant to §504.053(b) of the Texas Labor Code, this RME is necessary to resolve an issue relating to the entitlement to or amount of income benefits as required by §504.053(c)(1) of the Texas Labor Code.
•I am authorized to act on behalf of the insurance carrier.
I understand that misrepresenting a workers’ compensation claim may result in enforcement action including administrative penalties and fines.
31. |
Signature of Adjuster or Authorized Insurance Carrier Representative |
For |
|
|
|
32. |
Printed Name of Adjuster or Authorized Insurance Carrier Representative |
|
33. Title of Adjuster or Authorized Insurance Carrier Representative
34. Date of Signature
DWC022 Rev. 07/11 |
Page 1 of 3 |
|
|
|
|
|
DWC022 |
|
|
|
|
||
|
REQUEST FOR RME: APPROPRIATENESS OF HEALTH CARE RECEIVED (Complete Sections VII and VIII) |
||||
|
VII. EXAMINATION INFORMATION |
|
|
||
|
35. |
Examining RME Doctor's Name |
|
36. RME Doctor’s Mailing Address (Street or PO Box, City State Zip) |
37. RME Doctor’s License Number |
|
|
|
|
|
|
|
38. |
RME Doctor's Telephone Number |
|
39. Examination Location (Street, City State Zip) |
40. Date and Time of Appointment |
|
( |
) |
|
|
|
41. Date of Prior Examination
42. Prior Examining Doctor's Name
43. If different doctors are named in Boxes 35 and 42, explain the reason for requesting a different doctor.
44. Does the claim involve medical benefits provided through a Certified Health Care Network?
Yes
No If yes, provide the name of the network.
45.Does the claim involve medical benefits provided through a political subdivision pursuant to §504.053(b)(2) of the Texas Labor Code, relating to directly contracting with health care providers or contracting through a health benefits pool? Yes No
If yes, provide the name of the health care plan.
46.Are the employee’s address (Box 3) and the examination location (Box 39) more than 75 miles apart? If yes, explain why the employee is being required to travel more than 75 miles for the examination.
Yes
No
VIII. INSURANCE CARRIER CERTIFICATION
47.I hereby certify the following:
•This request is complete and accurate.
•I have obtained the injured employee’s agreement or attempted to obtain the injured employee’s agreement for an examination under Texas Labor Code §408.004 (Appropriateness of Health Care Examination) as follows:
Check ONLY ONE box below as applicable and provide date(s) as indicated for that box:
Injured employee/attorney notified insurance carrier of agreement to attend examination by carrier’s doctor on (mm/dd/yyyy) Injured employee/attorney notified insurance carrier of
Sent to injured employee/attorney on (mm/dd/yyyy) |
|
and no reply received as of (mm/dd/yyyy) |
•The insurance carrier will pay reasonable expenses incident to the examination of the injured employee.
•The selected doctor does not have a disqualifying association.
•I am authorized to act on behalf of the insurance carrier.
I understand that misrepresenting a workers’ compensation claim may result in enforcement action including administrative penalties and fines.
48. Signature of Adjuster or Authorized Insurance Carrier Representative
49. Date of Signature
50. Printed Name of Adjuster or Authorized Insurance Carrier Representative
51. Title of Person Signing
IX. INJURED EMPLOYEE
52. Complete this section and return a copy of this form to the insurance carrier ONLY if Section VII above has been completed.
I agree
I do not agree - to attend the requested examination to determine whether health care I have received was appropriate.
NOTE: If you agree, you must attend the examination at the time and location scheduled. If you do not agree, the insurance carrier will submit the request to
53. Signature of Injured Employee or Injured Employee’s Attorney/Representative
For
54.Printed Name of Injured Employee or Injured Employee’s Attorney/Representative
55.Date of Signature
NOTE: With few exceptions, upon your request, you are entitled to be informed about information
DWC022 Rev. 07/11 |
Page 2 of 3 |
DWC022
Information for the Injured Employee
For what purposes may a Required Medical Examination be requested?
DWC
•Request for Order (Evaluation of Designated Doctor Determination): If you have been examined by a Designated Doctor, the insurance carrier may ask
•Request for Agreement/Order (Appropriateness of Health Care Received): The insurance carrier may use the form to request your agreement to attend an RME to determine whether health care you have received was appropriate. You have 15 days from the date the carrier sent the request to you to complete Section IX. INJURED EMPLOYEE
Exception for Network Claims: If you received medical benefits through a certified workers’ compensation health care network, the insurance carrier is not permitted to request an RME on the appropriateness of health care received.
Exception for Certain Political Subdivision Claims: If you received medical benefits through a political subdivision pursuant to §504.053(b)(2) of the Texas Labor Code, relating to directly contracting with health care providers or contracting through a health benefits pool, the insurance carrier is not permitted to request an RME unless the RME is necessary to resolve a question relating to the entitlement to or amount of income benefits.
How often can a Required Medical Examination be performed?
An RME to determine appropriateness of health care received may not be performed more than once every 180 days. Examinations to evaluate a Designated Doctor determination may be performed more frequently. After you have received Supplemental Income Benefits for eight quarters, an RME to evaluate a Designated Doctor determination regarding your ability to
What will
Within 7 days of receiving the insurance carrier’s request for an RME,
If
NOTE: If the request is approved, your failure to attend the scheduled RME may be considered an administrative violation and may result in suspension of temporary income benefits, if applicable. You may request that your treating doctor attend the RME.
If
Can the RME appointment be rescheduled?
If you cannot attend an RME, you must contact the doctor’s office to reschedule the examination at least 24 hours in advance. The rescheduled appointment must be no later than 7 days after the original appointment unless you and the doctor agree on a different date that is no later than 30 days after the original appointment.
Questions / Information Regarding Travel Reimbursement
If you have questions regarding this form, need to request an accommodation under Title II of the Americans with Disabilities Act (ADA), or need information about reimbursement of travel expenses, contact
Instructions for the Insurance Carrier
RME regarding Evaluation of Designated Doctor Determination
•After completing Sections I, II, and III, complete Sections IV, V and VI regarding an Evaluation of Designated Doctor Determination RME.
•Check the applicable box(es) in Section V, Box 29 to describe the reason(s) for the examination.
•Fax the request to
RME regarding Appropriateness of Health Care Received
•After completing Sections I, II, and III, complete Section VII regarding an Appropriateness of Health Care Received RME.
•Attempt to obtain agreement by sending the form to the injured employee and the injured employee’s attorney or representative, if any.
•Upon obtaining the employee’s answer in writing or by telephone or after 15 days with no response, complete Section VIII. In this section you must indicate whether the injured employee agreed, refused to agree, or failed to respond to the request.
•Fax the request to
DWC022 Rev. 07/11 |
Page 3 of 3 |
| Fact Name | Details |
|---|---|
| Form Purpose | The DWC022 form is used to request a Required Medical Examination (RME) to assess an injured employee's medical condition and treatment appropriateness. |
| Governing Law | This form is governed by the Texas Labor Code, specifically §408.004 and §504.053. |
| Submission Deadline | Employees have 15 days from receiving the request to respond regarding their agreement to attend the examination. |
| Examination Frequency | An RME for appropriateness of health care can occur no more than once every 180 days, while evaluations of Designated Doctor determinations may happen more frequently. |
| Travel Distance | If the employee's address and the examination location are over 75 miles apart, an explanation is required in the form. |
| Insurance Carrier Certification | The insurance carrier must certify that the request is complete, accurate, and that the selected doctor has no disqualifying associations. |
| Rescheduling | If unable to attend, the employee must contact the doctor's office at least 24 hours in advance to reschedule, with a new appointment occurring within 7 days. |
| Travel Reimbursement | Employees can request travel reimbursement using DWC-Form 048, available through the Texas Department of Insurance website. |
Completing the Texas DWC022 form is an important step in the process of requesting a Required Medical Examination (RME). This form gathers essential information about the employee, employer, insurance carrier, and the medical examination itself. Follow these steps to ensure that you fill out the form accurately and completely.
Once you have filled out the form, review it carefully to ensure all sections are complete and accurate. After that, submit the form to the appropriate parties as instructed. Keeping a copy for your records is also a good practice.
What is the Texas DWC022 form?
The Texas DWC022 form is a document used in the workers' compensation process in Texas. It is specifically a request for a Required Medical Examination (RME) by the insurance carrier. This examination can address issues related to the evaluation of a designated doctor’s determination or assess the appropriateness of health care received by an injured employee.
When is the DWC022 form required?
The form is necessary when an insurance carrier wants to request an RME for an injured employee. This can occur in two main scenarios: to evaluate a designated doctor's findings or to determine if the health care received was appropriate. The request must be submitted to the Texas Department of Insurance, Division of Workers’ Compensation (TDI-DWC).
What information do I need to provide on the form?
The DWC022 form requires various details, including:
How often can a Required Medical Examination be performed?
An RME to assess the appropriateness of health care received can only occur once every 180 days. However, examinations related to a designated doctor’s determination can be more frequent. After receiving Supplemental Income Benefits for eight quarters, an RME regarding the ability to return to work may be conducted no more than once a year.
What happens after I submit the DWC022 form?
Once TDI-DWC receives the insurance carrier’s request for an RME, they will review it within seven days. If approved, TDI-DWC will issue an order requiring the injured employee to attend the examination. If the request is denied, the employee will not be required to attend.
Can I reschedule my RME appointment?
If you cannot attend the RME, you must contact the doctor's office to reschedule at least 24 hours in advance. The new appointment must take place within seven days of the original date, unless you and the doctor agree on a different date, which should not exceed 30 days from the original appointment.
What should I do if I have questions about travel reimbursement?
If you have questions regarding travel reimbursement or need to request accommodations under the Americans with Disabilities Act (ADA), you can contact TDI-DWC at (800) 252-7031. To request travel reimbursement, you will need to fill out the DWC-Form 048, which is available on the TDI website.
Filling out the Texas DWC022 form can be a daunting task, and mistakes can lead to delays or complications in the workers' compensation process. One common error is providing incorrect personal information. This includes the employee's name, Social Security number, or address. Even a small typo can cause significant issues, so it's crucial to double-check these details for accuracy.
Another frequent mistake involves failing to complete all necessary sections of the form. Each section serves a specific purpose, and incomplete information can result in the form being returned or rejected. It is essential to read the instructions carefully and ensure that every applicable section is filled out completely.
Many individuals also overlook the importance of signatures. The form requires signatures from both the insurance carrier representative and the injured employee or their attorney. Missing a signature can delay the process and may require resubmission. Always confirm that all required signatures are present before submitting the form.
Additionally, people sometimes neglect to provide explanations when required. For instance, if the employee's address and the examination location are more than 75 miles apart, an explanation is necessary. Failing to include this information can lead to confusion and may hinder the processing of the request.
Finally, some individuals misinterpret the purpose of the form. Understanding whether the request is for a Required Medical Examination (RME) regarding a designated doctor or the appropriateness of health care received is vital. Misunderstanding the purpose can lead to filling out the wrong sections or providing irrelevant information, complicating the process further.
The Texas DWC022 form is an important document in the workers' compensation process, specifically for requesting a Required Medical Examination (RME). Along with this form, there are several other documents that may be commonly used. Each of these documents serves a unique purpose in the claims process, helping to ensure that all necessary information is collected and reviewed.
Understanding these documents can help injured employees navigate the workers' compensation process more effectively. Each form plays a role in ensuring that the employee receives appropriate medical evaluation and support throughout their recovery journey.
The Texas DWC022 form serves specific purposes related to workers' compensation claims. Several other documents share similarities with the DWC022 form in terms of their function and the information they require. Below is a list of these similar documents:
When filling out the Texas DWC022 form, there are several important things to keep in mind. Here’s a list of what you should and shouldn't do:
This is not true. The DWC022 form is used for various purposes, including requesting a Required Medical Examination (RME) to evaluate medical benefits or the appropriateness of care received, regardless of whether benefits have been denied.
Submitting the form does not automatically mean an examination will take place. The Texas Department of Insurance, Division of Workers’ Compensation (TDI-DWC) reviews the request and decides whether to approve or deny it.
Employees actually have 15 days from the date they receive the request to complete the agreement section of the form and return it to the insurance carrier. Timely responses are crucial.
There are specific guidelines regarding how often an RME can be performed. For instance, an RME to determine the appropriateness of health care cannot occur more than once every 180 days.
The RME must be conducted by a doctor selected by the insurance carrier. Employees may not have the flexibility to choose their own doctor for this examination.
If an employee does not agree to attend the RME, the insurance carrier can still request TDI-DWC to issue an order requiring attendance. Noncompliance could lead to penalties.
Even if an employee has a treating physician, the DWC022 form may still be required for specific examinations related to the workers' compensation claim, especially if the insurance carrier needs further evaluation.
In fact, the insurance carrier is required to pay reasonable expenses related to the examination. Employees should inquire about travel reimbursement using the appropriate forms.
The Texas DWC022 form is essential for requesting a Required Medical Examination (RME) to assess either the appropriateness of medical care received or to evaluate a Designated Doctor’s determination.
It is crucial to fill out all sections accurately. Missing information can delay the process and lead to complications in your workers' compensation claim.
Employees have a limited time frame of 15 days to respond to the request for agreement to attend the examination. Keeping a copy of the completed form for personal records is advisable.
If an employee cannot attend the scheduled examination, they must contact the doctor's office at least 24 hours in advance to reschedule, ensuring it is done within the specified time limits.