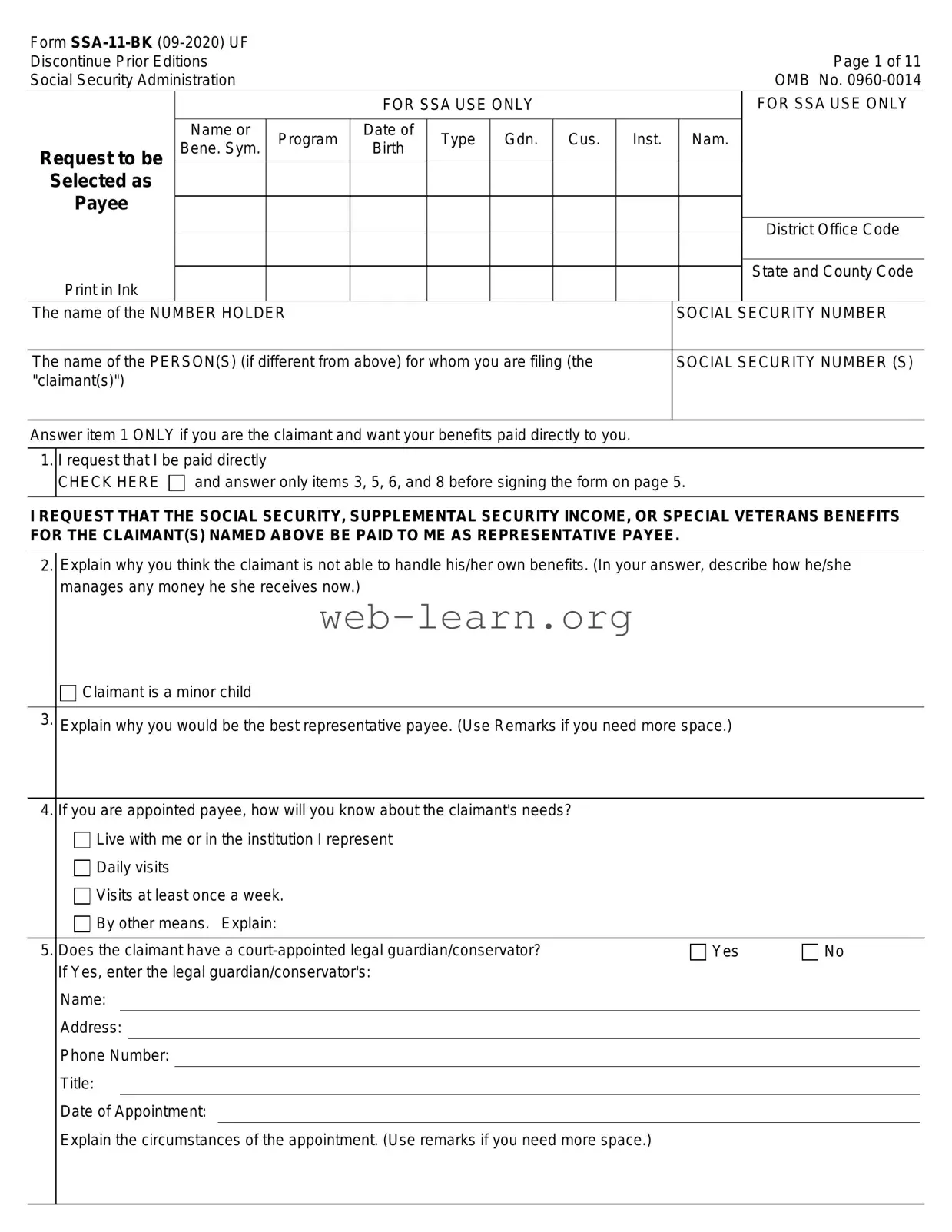
The SSA-11 form, also known as the Request to be Selected as Payee, is an important document for those who wish to manage Social Security benefits on behalf of someone else. This form is primarily used when an individual, referred to as the "claimant," cannot handle their own benefits due to various reasons, such as age or disability. The form requires the applicant to provide personal information about both themselves and the claimant, including Social Security numbers and living arrangements. It also asks for details on why the claimant is unable to manage their benefits and how the applicant plans to meet the claimant's needs. Furthermore, the SSA-11 includes questions regarding any legal guardianship and the applicant's relationship to the claimant. Understanding how to fill out this form accurately is crucial, as it ensures that benefits are directed to the right person and used for the claimant's needs. This article will delve into the key aspects of the SSA-11 form, guiding you through the application process and highlighting essential considerations for prospective payees.
Form |
|
|
|
|
|
|
|
Discontinue Prior Editions |
|
|
|
|
|
Page 1 of 11 |
|
Social Security Administration |
|
|
|
|
|
OMB No. |
|
|
|
|
FOR SSA USE ONLY |
|
|
FOR SSA USE ONLY |
|
|
|
|
|
|
|
|
|
|
Name or |
Program |
Date of |
Type Gdn. Cus. |
Inst. Nam. |
|
|
Request to be |
Bene. Sym. |
Birth |
|
||||
|
|
|
|
|
|
|
|
Selected as |
|
|
|
|
|
|
|
Payee |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
District Office Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Print in Ink |
|
|
|
|
|
|
State and County Code |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
The name of the NUMBER HOLDER |
|
|
|
SOCIAL SECURITY NUMBER |
|||
|
|
|
|||||
The name of the PERSON(S) (if different from above) for whom you are filing (the |
|
SOCIAL SECURITY NUMBER (S) |
|||||
"claimant(s)") |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Answer item 1 ONLY if you are the claimant and want your benefits paid directly to you.
1.I request that I be paid directly
CHECK HERE and answer only items 3, 5, 6, and 8 before signing the form on page 5.
I REQUEST THAT THE SOCIAL SECURITY, SUPPLEMENTAL SECURITY INCOME, OR SPECIAL VETERANS BENEFITS FOR THE CLAIMANT(S) NAMED ABOVE BE PAID TO ME AS REPRESENTATIVE PAYEE.
2.Explain why you think the claimant is not able to handle his/her own benefits. (In your answer, describe how he/she manages any money he she receives now.)
Claimant is a minor child
3.Explain why you would be the best representative payee. (Use Remarks if you need more space.)
4.If you are appointed payee, how will you know about the claimant's needs?
Live with me or in the institution I represent |
|
|
|
||||
Daily visits |
|
|
|
||||
Visits at least once a week. |
|
|
|
||||
By other means. Explain: |
|
|
|
||||
|
|
|
|
|
|
|
|
5. Does the claimant have a |
Yes |
No |
|||||
If Yes, enter the legal guardian/conservator's: |
|
|
|
||||
Name: |
|
|
|
|
|||
Address: |
|
|
|
|
|||
Phone Number: |
|
|
|
|
|||
Title: |
|
|
|
|
|||
Date of Appointment: |
|
|
|
|
|||
Explain the circumstances of the appointment. (Use remarks if you need more space.) |
|
|
|
||||
Form |
Page 2 of 11 |
|
6. (a) Where does the claimant live? |
|
|
|
Alone |
|
|
In my home (Go to (b).) |
In a public institution (Go to (c).) |
|
With a relative (Go to (b).) |
In a private institution (Go to (c).) |
|
With someone else (Go to (b).) |
In a nursing home (Go to (c).) |
|
In a board and care facility (Go to (b).) |
In the institution I represent (Go to (c).) |
|
|
|
|
(b) Enter the names and relationships of any other people who live with the claimant. |
|
|
|
|
|
NAME |
RELATIONSHIP |
|
|
|
|
|
|
|
|
|
|
|
|
(c) Enter the claimant's residence and mailing addresses (if different from yours).
Residence: |
Mailing: |
Telephone |
|
|
Number |
|
|
|
(d) Do you expect the claimant's living arrangements to change in the next year? |
Yes |
No |
If Yes, explain what changes are expected and when they will occur. (Use Remarks if you need more space.)
7. If you are applying on behalf of minor child(ren) and you are not the parent, |
|
|||
Is the child(ren) in foster care? |
Yes |
No |
||
Does the child(ren) have a living natural or adoptive parent? |
Yes |
No |
||
If yes, enter: (a) Name of parent |
|
|
|
|
(b) Address of parent |
|
|
||
(c) Telephone number |
|
|
|
|
(d) Does the parent show interest in the child? |
Yes |
No |
||
Please explain: |
|
|
||
8.List the names and relationship of any (other) relatives or close friends who have provided support and/or show active interest with the claimant. Describe the type and amount of support and/or how interest is displayed.
|
NAME |
ADDRESS/PHONE NO. |
RELATIONSHIP |
DESCRIBE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Form |
Page 3 of 11 |
9.Check the block that describes your relationship to the claimant.
(a)Official of bank, agency or institution with responsibility for the person. Enter below which you represent:
Bank |
State, county, or local government agency |
Social Agency |
Public Official |
|
Institution: |
|
|
|
|
Federal |
State/Local |
Private |
|
|
Private proprietary institution. Is the institution licensed under State law? |
Yes |
No |
||
IF (a) ABOVE CHECKED, COMPLETE ONLY QUESTIONS 10 AND 11 AND SIGN THE FORM ON PAGE 5.
(b) Parent
(c) Spouse
(d) Other Relative - Specify
(e) Legal Representative
(f) Board and Care Home Operator
(g) Other Individual - Specify
IF (b), (c), (d), or (e) ABOVE CHECKED, GO ON TO QUESTION 12
10. Does the claimant owe you/your organization any money now or will he/she owe you money in the future? Yes No
If Yes, enter the amount he/she owes you/your organization, the date(s) was/will be incurred and describe why the debt was/ will be incurred.
INFORMATION ABOUT INSTITUTIONS, AGENCIES, AND BANKS APPLYING TO BE REPRESENTATIVE PAYEE
11.(a) Enter the name of the institution
(b) Enter the EIN of the institution
INFORMATION ABOUT INDIVIDUALS APPLYING TO BE REPRESENTATIVE PAYEE |
||||||
|
|
|
|
|
|
|
12. Enter: Your name |
|
|
|
|
||
Date of birth |
|
Social Security Number |
|
|
||
Any other name you have used |
|
|
|
|
||
Other SSN's you have used |
|
|
|
|
||
13.How long have you known the claimant?
14.If the claimant lives with you, who takes care of the claimant when work or other activity takes you away from home? What is his/her relationship to the claimant?
15.(a) Main source of your income
Employed (answer (b) below) |
|
|||||||
|
) |
|||||||
Social Security benefits (Claim Number |
|
) |
||||||
Pension (describe |
|
) |
||||||
Supplemental Security Income payments (Claim Number |
|
) |
||||||
Temporary Assistance For Needy Families (TANF |
|
) |
||||||
Other State or Public Assistance (describe |
|
) |
||||||
Other (describe |
) |
|||||||
|
|
|
|
|
|
|
|
|
(b) Enter your employer's name and address: |
|
|||||||
How long have you been employed by this employer?
(If less than 1 year, enter name and address of previous employer in Remarks.)
Form |
Page 4 of 11 |
||||||||||||||
16. |
Do you give Social Security permission to conduct a criminal background check on you? |
Yes |
No |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
17. |
(a) Have you ever been convicted of a felony? |
Yes |
No |
||||||||||||
|
If Yes: What was the crime? |
|
|
|
|
||||||||||
|
On what date were you convicted? |
|
|
|
|
||||||||||
|
What was your sentence? |
|
|
|
|
||||||||||
|
If imprisoned, when were you released? |
|
|
|
|
||||||||||
|
If probation was ordered, when did/will your probation end? |
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(b) Have you ever been convicted of any offense under federal or state law which resulted in imprisonment |
Yes |
No |
||||||||||||
|
for more than one year? |
|
|
|
|||||||||||
|
If Yes: What was the crime? |
|
|
|
|
||||||||||
|
On what date were you convicted? |
|
|
|
|
||||||||||
|
What was your sentence? |
|
|
|
|
||||||||||
|
If imprisoned, when were you released? |
|
|
|
|
||||||||||
|
If probation was ordered, when did/will your probation end? |
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18. |
Do you have any unsatisfied FELONY warrants (or in jurisdictions that do not define crimes as felonies, a crime punishable |
||||||||||||||
|
by death or imprisonment exceeding 1 year) for your arrest? |
Yes |
No |
||||||||||||
|
If Yes: Date of Warrant |
|
|
|
|
||||||||||
|
State where warrant was issued |
|
|
|
|
||||||||||
|
|
|
|
|
|||||||||||
19. |
How long have you lived at your current address? (Give Date MM/YY) |
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REMARKS: (This space may be used for explaining any answers to the questions. If you need more space, attach a separate sheet.)
Form |
Page 5 of 11 |
PLEASE READ THE FOLLOWING INFORMATION CAREFULLY BEFORE SIGNING THIS FORM |
|
I/my organization:
•Must use all payments made to me/my organization as the representative payee for the claimant's current needs or (if not currently needed) save them for his/her future needs.
•May be held liable for repayment if I/my organization misuse the payments or if I/my organization am/is at fault for any overpayment of benefits.
•May be punished under Federal law by fine, imprisonment or both if I/my organization am/is found guilty of misuse of Social Security or SSI benefits.
I/my organization will:
•Use the payments for the claimant's current needs and save any currently unneeded benefits for future use.
•File an accounting report on how the payments were used, and make all supporting records available for review if requested by the Social Security Administration.
•Reimburse the amount of any loss suffered by any claimant due to misuse of Social Security or SSI funds by me/my organization.
•Notify the Social Security Administration when the claimant dies, leaves my/my organization's custody or otherwise changes his/her living arrangements or he/she is no longer my/my organization's responsibility.
•Comply with the conditions for reporting certain events (listed on the attached sheets(s) which I/my organization will keep for my/my organization's records) and for returning checks the claimant is not due.
•File an annual report of earnings if required.
•Notify the Social Security Administration as soon as I/my organization can no longer act as representative payee or the claimant no longer needs a payee.
I declare under penalty of perjury that I have examined all the information on this form, and on any accompanying statements or forms, and it is true and correct to the best of my knowledge.
SIGNATURE OF APPLICANT
Signature (First name, middle initial, last name) (Write in ink)
DATE (MM/DD/YYYY)
Telephone number(s) at which you may be contacted during the day
Print Your Name & Title (if a representative or employee of an institution/organization)
Mailing Address (Number and street, Apt. No., P.O. Box, or Rural Route)
City and State
ZIP Code
Name of County
Residence Address (Number and street, Apt. No., P.O. Box, or Rural Route)
City and State |
ZIP Code |
Name of County |
Witnesses are only required if this application has been signed by mark (X) above. If signed by mark (X), two witnesses to the signing who know the applicant making the request must sign below, giving their full addresses.
1. Signature of Witness
2. Signature of Witness
Address (Number and street, City, State, and ZIP Code)
Address (Number and street, City, State, and ZIP Code)
Form |
Page 6 of 11 |
SOCIAL SECURITY
Information for Representative Payees Who Receive Social Security Benefits
YOU MUST NOTIFY THE SOCIAL SECURITY ADMINISTRATION PROMPTLY IF ANY OF THE FOLLOWING EVENTS OCCUR AND PROMPTLY RETURN ANY PAYMENT TO WHICH THE CLAIMANT IS NOT ENTITLED:
•the claimant DIES (Social Security entitlement ends the month before the month the claimant dies);
•the claimant MARRIES, if the claimant is entitled to child's, widow's, mother's, father's, widower's or parent's benefits, or to wife's or husband's benefits as divorced wife/husband, or to special age 72 payments;
•the claimant's marriage ends in DIVORCE or ANNULMENT, if the claimant is entitled to wife's, husband's or special age 72 payments;
•the claimant's SCHOOL ATTENDANCE CHANGES if the claimant is age 18 or over and entitled to child's benefits as a full time student
•the claimant is entitled as a stepchild and the parents DIVORCE (benefits terminate the month after the month the divorce becomes final);
•the claimant is under FULL RETIREMENT AGE (FRA) and WORKS for more than the annual limit (as determined each year) or more than the allowable time (for work outside the United States);
•the claimant receives a GOVERNMENT PENSION or ANNUITY or the amount of the annuity changes, if the claimant is entitled to husband's, widower's, or divorced spouse's benefit's;
•the claimant leaves your custody or care or otherwise CHANGES ADDRESS;
•the claimant NO LONGER HAS A CHILD IN CARE, if he/she is entitled to benefits because of caring for a child under age 16 or who is disabled;
•the claimant is confined to jail, prison, penal institution or correctional facility;
•the claimant is confined to a public institution by court order in connection WITH A CRIME.
•the claimant has an UNSATISFIED FELONY WARRANT (or in jurisdictions that do not define crimes as felonies, a crime punishable by death or imprisonment exceeding 1 year) issue for his/her arrest;
•the claimant is violating a condition of probation or parole under State or Federal law.
IF THE CLAIMANT IS RECEIVING DISABILITY BENEFITS, YOU MUST ALSO REPORT IF:
•the claimant's MEDICAL CONDITION IMPROVES;
•the claimant STARTS WORKING;
•the claimant applies for or receives WORKER'S COMPENSATION BENEFITS, Black Lung Benefits from the Department of Labor, or a public disability benefit;
•the claimant is DISCHARGED FROM THE HOSPITAL (if now hospitalized).
IF THE CLAIMAINT IS RECEIVING SPECIAL AGE 72 PAYMENTS, YOU MUST ALSO REPORT IF:
•the claimant or spouse becomes ELIGIBLE FOR PERIODIC GOVERNMENTAL PAYMENTS, whether from the U.S. Federal government or from any State or local government;
•the claimant or spouse receives SUPPLEMENTAL SECURITY INCOME or PUBLIC ASSISTANCE CASH BENEFITS;
•the claimant or spouse MOVES outside the United States (the 50 States, the District of Columbia and the Northern Mariana Islands).
In addition to these events about the claimant, you must also notify us if:
•YOU change your address;
•YOU are convicted of a felony or any offense under State or Federal law which results in imprisonment for more than 1 year;
•YOU have a UNSATISFIED FELONY WARRANT (or in jurisdictions that do not define crimes as felonies, a crime punishable by death or imprisonment exceeding 1 year) issued for your arrest.
BENEFITS MAY STOP IF ANY OF THE ABOVE EVENTS OCCUR. You should read the informational booklet we will send you to see how these events affect benefits. You may make your reports by telephone, mail, or in person.
REMEMBER:
•payments must be used for the claimant's current needs or saved if not currently needed;
•you may be held liable for repayment of any payments not used for the claimant's needs or of any over payment that occurred due to your fault;
•you must account for benefits when so asked by the Social Security Administration. You will keep records of how benefits were spent so you can provide us with correct accounting;
•to tell us as soon as you know you will no longer be able to act as representative payee or the claimant no longer needs a payee.
Keep in mind that benefits may be deposited directly into an account set up for the claimant with you as payee. As soon as you set up such an account, contact us for more information about receiving the claimant's payments using direct deposit.
Form |
|
|
Page 7 of 11 |
|
|
|
A REMINDER TO PAYEE APPLICANTS |
|
|
|
|
|
|
|
Telephone |
Before you Receive a |
|
SSA Office |
Date Request |
Decision Notice |
|
|
Received |
|
Number(s) to Call |
|
|
||
if you have a |
|
|
|
|
Question or |
After you Receive a |
|
|
|
Something to |
Decision Notice |
|
|
|
Report |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RECEIPT FOR YOUR REQUEST |
|
Your request for Social Security benefits on behalf of the individual(s) named below has been received and will be processed as quickly as possible.
You should hear from us within days after you have given us all the information we requested. Some claims may take longer if additional information is needed.
In the meantime, if you change your address, or if there is some other change that may affect the benefits payable,
you - or someone for you - should report the change. The changes to be reported are listed on the reverse.
Always give us the claim number of the beneficiary when writing or telephoning about the claim.
If you have any questions about this application, we will be glad to help you.
BENEFICIARY
SOCIAL SECURITY CLAIM NUMBER
Privacy Act Statement
Collection and Use of Personal Information
Sections 205(a), 205(j), and 1631(a) of the Social Security Act, as amended, allow us to collect this information. Furnishing us this information is voluntary. However, failing to provide all or part of the information may prevent an accurate and timely decision on your request for selection as a representative payee.
We will use the information to determine your eligibility to serve as a representative payee. We may also share your information for the following purposes, called routine uses:
•To contractors and other Federal agencies, as necessary, for the purpose of assisting the Social Security Administration (SSA) in the efficient administration of its programs;
•To agencies or entities who have a written agreement with SSA, to perform reviews of the representative payee program and to provide training, administrative oversight, technical assistance, and other support for the program review; and
•To third parties, contractors, or other Federal agencies, as necessary, to conduct criminal background checks and to obtain criminal history information on representative payees and representative payee applicants.
In addition, we may share this information in accordance with the Privacy Act and other Federal laws. For example, where authorized, we may use and disclose this information in computer matching programs, in which our records are compared with other records to establish or verify a person's eligibility for Federal benefit programs and for repayment of incorrect or delinquent debts under these programs.
A list of additional routine uses is available in our Privacy Act System of Records Notices (SORN)
Paperwork Reduction Act Statement
This information collection meets the requirements of 44 U.S.C. § 3507, as amended by section 2 of The Paperwork Reduction Act of 1995. You do not need to answer these questions unless we display a valid Office of Management and Budget (OMB) control number. We estimate that it will take about 11 minutes to read the instructions, gather the facts, and answer the questions. Send only comments relating to our time estimate above to: SSA, 6401 Security Blvd, Baltimore, MD

Form |
Page 8 of 11 |
SUPPLEMENTAL SECURITY INCOME
Information for Representative Payees Who Receive Social Security Benefits
YOU MUST NOTIFY THE SOCIAL SECURITY ADMINISTRATION PROMPTLY IF ANY OF THE FOLLOWING EVENTS OCCUR AND PROMPTLY RETURN ANY PAYMENT TO WHICH THE CLAIMANT IS NOT ENTITLED:
•the claimant or any member of the claimant's household DIES (SSI eligibility ends with the month in which the claimant dies);
•the claimant's HOUSEHOLD CHANGES (someone moves in/out of the place where the claimant lives);
•the claimant LEAVES THE U.S. (the 50 states, the District of Columbia, and the Northern Mariana Islands) for 30 consecutive days or more;
•the claimant MOVES or otherwise changes the place where he/she actually lives (including adoption, and whereabouts unknown);
•the claimant is ADMITTED TO A HOSPITAL, skilled nursing facility, nursing home, intermediate care facility, or other institution; • the INCOME of the claimant or anyone in the claimant's household CHANGES (this includes income paid by an organization or employer, as well as monetary benefits from other sources);
•the RESOURCES of the claimant or anyone in the claimant's household CHANGES (this includes when conserved funds reach over $2,000);
•the claimant or anyone in the claimant's household MARRIES;
•the marriage of the claimant or anyone in the claimant's household ends in DIVORCE or ANNULMENT;
•the claimant SEPARATES from his/her spouse;
•the claimant is confined to jail, prison, penal institution or correctional facility;
•the claimant is confined to a public institution by court order in connection WITH A CRIME;
•the claimant has an UNSATISFIED FELONY WARRANT (or in jurisdictions that do not define crimes as felonies, a crime punishable by death or imprisonment exceeding 1 year) issued for his/her arrest;
•the claimant is violating a condition of probation or parole under State or Federal law.
IF THE CLAIMANT IS RECEIVING PAYMENTS DUE TO DISABILITY OR BLINDNESS, YOU MUST ALSO REPORT IF:
•the claimant's MEDICAL CONDITION IMPROVES;
•the claimant GOES TO WORK;
•the claimant's VISION IMPROVES, if the claimant is entitled due to blindness;
In addition to these events about the claimant, you must also notify us if:
•YOU change your address;
•YOU are convicted of a felony or any offense under State or Federal law which results in imprisonment for more than 1 year;
•YOU have an UNSATISFIED FELONY WARRANT (or in jurisdictions that do not define crimes as felonies, a crime punishable by death or imprisonment exceeding 1 year) issued for your arrest.
PAYMENT MAY STOP IF ANY OF THE ABOVE EVENTS OCCUR. You should read the informational booklet we will send you to see how these events affect benefits. You may make your reports by telephone, mail or in person.
REMEMBER:
•payments must be used for the claimant's current needs or saved if not currently needed. (Savings are considered resources and may affect the claimant's eligibility to payment.);
•you may be held liable for repayment of any payments not used for the claimant's needs or of any overpayment that occurred due to your fault;
•you must account for benefits when so asked by the Social Security Administration. You will keep records of how benefits were spent so you can provide us with a correct accounting;
•to let us know as soon as you know you are unable to continue as representative payee or the claimant no longer needs a payee
•you will be asked to help in periodically redetermining the claimant's continued eligibility or payment. You will need to keep evidence to help us with the redetermination (e.g., evidence of income and living arrangements).
•you may be required to obtain medical treatment for the claimant's disabling condition if he/she is eligible under the childhood disability provision.
Keep in mind that payments may be deposited directly into an account set up for the claimant with you as payee. As soon as you set up such an account, contact us for more information about receiving the claimant's payments using direct deposit.
Form |
|
|
Page 9 of 11 |
|
|
|
A REMINDER TO PAYEE APPLICANTS |
|
|
|
|
|
|
|
Telephone |
Before you Receive a |
|
SSA Office |
Date Request |
Decision Notice |
|
|
Received |
|
Number(s) to Call |
|
|
||
if you have a |
|
|
|
|
Question or |
After you Receive a |
|
|
|
Something to |
Decision Notice |
|
|
|
Report |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RECEIPT FOR YOUR REQUEST |
|
Your request for SSI payments on behalf of the individual(s) named below has been received and will be processed as quickly as possible.
You should hear from us within days after you have given us all the information we requested. Some claims may take longer if additional information is needed.
In the meantime, if you change your address, or if there is some other change that may affect the benefits payable,
you - or someone for you - should report the change. The changes to be reported are listed on the reverse.
Always give us the claim number of the beneficiary when writing or telephoning about the claim.
If you have any questions about this application, we will be glad to help you.
BENEFICIARY
SOCIAL SECURITY CLAIM NUMBER
Privacy Act Statement
Collection and Use of Personal Information
Sections 205(a), 205(j), and 1631(a) of the Social Security Act, as amended, allow us to collect this information. Furnishing us this information is voluntary. However, failing to provide all or part of the information may prevent an accurate and timely decision on your request for selection as a representative payee.
We will use the information to determine your eligibility to serve as a representative payee. We may also share your information for the following purposes, called routine uses:
•To contractors and other Federal agencies, as necessary, for the purpose of assisting the Social Security Administration (SSA) in the efficient administration of its programs;
•To agencies or entities who have a written agreement with SSA, to perform reviews of the representative payee program and to provide training, administrative oversight, technical assistance, and other support for the program review; and
•To third parties, contractors, or other Federal agencies, as necessary, to conduct criminal background checks and to obtain criminal history information on representative payees and representative payee applicants.
In addition, we may share this information in accordance with the Privacy Act and other Federal laws. For example, where authorized, we may use and disclose this information in computer matching programs, in which our records are compared with other records to establish or verify a person's eligibility for Federal benefit programs and for repayment of incorrect or delinquent debts under these programs.
A list of additional routine uses is available in our Privacy Act System of Records Notices (SORN)
Paperwork Reduction Act Statement
This information collection meets the requirements of 44 U.S.C. § 3507, as amended by section 2 of The Paperwork Reduction Act of 1995. You do not need to answer these questions unless we display a valid Office of Management and Budget (OMB) control number. We estimate that it will take about 11 minutes to read the instructions, gather the facts, and answer the questions. Send only comments relating to our time estimate above to: SSA, 6401 Security Blvd, Baltimore, MD
Form |
Page 10 of 11 |
SPECIAL BENEFITS FOR WORLD WAR II VETERANS
Information for Representative Payees Who Receive Special Benefits for WW II Veterans
YOU MUST NOTIFY THE SOCIAL SECURITY ADMINISTRATION PROMPTLY IF ANY OF THE FOLLOWING EVENTS OCCUR AND PROMPTLY RETURN ANY PAYMENT TO WHICH THE CLAIMANT IS NOT ENTITLED:
•the claimant DIES (special veterans entitlement ends the month after the claimant dies);
•the claimant returns to the United States for a calendar month or longer;
•the claimant moves or changes the place where he/she actually lives;
•the claimant receives a pension, annuity or other recurring payment (includes workers' compensation, veterans benefits or disability benefits), or the amount of the annuity changes;
•the claimant is or has been deported or removed from U.S.;
•the claimant has an UNSATISFIED FELONY WARRANT (or in jurisdictions that do not define crimes as felonies, a crime punishable by death or imprisonment exceeding 1 year) issued for his/her arrest;
•the claimant is violating a condition of probation or parole under State or Federal law.
In addition to these events about the claimant, you must also notify us if:
•YOU change your address;
•YOU are convicted of a felony or any offense under State or Federal law which results in imprisonment for more than 1 year;
•YOU have an UNSATISFIED FELONY WARRANT (or in jurisdictions that do not define crimes as felonies, a crime punishable by death or imprisonment exceeding 1 year) issued for your arrest.
BENEFITS MAY STOP IF ANY OF THE ABOVE EVENTS OCCUR. You can make your reports by telephone, mail or in person. You can contact any U.S. Embassy, Consulate, Veterans Affairs Regional Office in the Philippines or any U.S. Social Security Office.
REMEMBER:
•payments must be used for the claimant's current needs or saved if not currently needed;
•you may be held liable for repayment of any payments not used for the claimant's needs or of any overpayment that occurred due to your fault;
•you must account for benefits when so asked by the Social Security Administration. You will keep records of how benefits were spent so you can provide us with a correct accounting;
•to let us know, as soon as you know you are unable to continue as representative payee or the claimant no longer needs a payee.
| Fact Name | Description |
|---|---|
| Purpose of SSA-11 | The SSA-11 form is used to request to be appointed as a representative payee for someone who is unable to manage their Social Security benefits. |
| Eligibility Criteria | Individuals applying to be a payee must demonstrate that the claimant cannot handle their own benefits, often due to age or disability. |
| Required Information | The form requires details about the claimant, including their living situation and any legal guardianship arrangements. |
| Signature Requirement | Applicants must sign the form in ink, confirming that the information provided is accurate to the best of their knowledge. |
| Witnesses | If the applicant signs by mark (X), two witnesses must sign the form, providing their addresses as well. |
| Legal Obligations | Payees must use benefits for the claimant's current needs and may be liable for repayment if funds are misused. |
| Reporting Changes | Payees are required to notify the Social Security Administration of any significant changes in the claimant's circumstances, such as death or change of address. |
| Background Check | Applicants must consent to a criminal background check, which is part of the vetting process for potential payees. |
| State-Specific Forms | Some states may have additional requirements or forms that must be submitted alongside the SSA-11, governed by local laws. |
| Form Updates | The SSA-11 form is periodically updated, and older editions should be destroyed to avoid confusion. |
Filling out the SSA-11 form is an important step in the process of requesting to be a representative payee for someone who cannot manage their own benefits. After completing the form, it will need to be submitted to the Social Security Administration for review. Ensure that all information is accurate and complete to avoid delays.
Form SSA-11 is a request to be selected as a representative payee for someone receiving Social Security benefits. This form is used when an individual believes that a claimant is unable to manage their own benefits due to various reasons, such as age or disability.
The form can be filled out by anyone who wishes to act as a representative payee for a claimant. This includes parents, guardians, or individuals from institutions responsible for the claimant’s care. It is important that the person filling out the form has a genuine interest in the claimant's well-being.
The form requires various details, including:
A representative payee is needed when a claimant cannot manage their benefits due to reasons like mental incapacity, severe physical limitations, or being a minor. The payee ensures that benefits are used for the claimant's current needs and future expenses.
To become a representative payee, an individual must complete Form SSA-11 and provide necessary information about their relationship to the claimant. The Social Security Administration will review the application and determine if the individual is suitable for the role.
A representative payee is responsible for using the benefits to meet the claimant's needs, keeping accurate records of how the funds are spent, and reporting any changes in circumstances to the Social Security Administration. Misuse of funds can lead to serious legal consequences.
Yes, a representative payee can be changed if it is determined that the current payee is no longer suitable or if the claimant's needs change. The new payee must submit a new Form SSA-11 for approval.
If the claimant dies, the representative payee must notify the Social Security Administration immediately. Benefits will stop for the month prior to the claimant’s death, and any unspent funds must be returned.
Form SSA-11 can be obtained online from the Social Security Administration's website or by visiting a local Social Security office. It is important to ensure that you are using the most current version of the form.
Filling out the SSA-11 form can be a straightforward process, but many people make common mistakes that can delay their application. One frequent error is failing to provide complete and accurate information. When applicants leave sections blank or provide vague answers, it can lead to confusion and additional requests for clarification from the Social Security Administration (SSA). Each question is designed to gather specific information, and incomplete responses can hinder the review process.
Another mistake is not clearly explaining the claimant's inability to manage their own benefits. The form asks for detailed explanations, yet some applicants provide minimal information. It is essential to describe the claimant's current financial situation and how they handle any money they receive. A thorough explanation helps the SSA understand why a representative payee is necessary.
Additionally, many applicants overlook the importance of providing accurate contact information. Failing to include a current phone number or mailing address can lead to missed communications from the SSA. If the SSA cannot reach the applicant for follow-up questions, it may result in delays or even denials of the application.
Some individuals also forget to check the appropriate boxes that indicate their relationship to the claimant. This oversight can create confusion about the applicant's role and responsibilities. It's important to ensure that the correct relationship is documented, as this helps establish the legitimacy of the payee's request.
Another common error involves not notifying the SSA of any changes in circumstances. If there are changes in the claimant's living situation or financial needs, these must be reported promptly. Failing to do so can lead to complications or even potential overpayments that the payee may be held responsible for repaying.
Moreover, applicants sometimes fail to sign and date the form correctly. An unsigned or improperly dated form will be rejected, causing unnecessary delays. It is crucial to double-check that all required signatures are present before submitting the application.
Lastly, some applicants neglect to read the instructions carefully. The SSA provides specific guidelines on how to fill out the form, and overlooking these can result in mistakes. Taking the time to review the instructions can help ensure that the application is completed correctly and submitted without issues.
The SSA-11 form, officially known as the Request to Be Selected as Payee, is utilized by individuals seeking to become representative payees for Social Security benefits. In conjunction with this form, several other documents may be necessary to ensure a complete application process. Below is a list of related forms and documents commonly required alongside the SSA-11 form.
Each of these forms and documents plays a critical role in the application process for Social Security benefits. They help ensure that the SSA has all necessary information to make informed decisions regarding eligibility and the appropriate allocation of benefits. Proper completion and submission of these documents can facilitate a smoother application experience for both claimants and their representative payees.
The SSA-11 form is a request to be selected as a representative payee for Social Security benefits. Several other documents serve similar purposes in different contexts. Here are nine documents that share similarities with the SSA-11 form:
Each of these forms plays a critical role in managing Social Security benefits and ensuring that the needs of claimants are adequately addressed.
When filling out the SSA-11 form, it's important to approach the process with care. Here are five things you should and shouldn't do to ensure your application is handled smoothly:
By following these guidelines, you can help ensure that your application process goes as smoothly as possible.
Understanding the SSA-11 form, which is used to request to be selected as a representative payee for Social Security benefits, can be challenging. Here are eight common misconceptions about this form:
By clarifying these misconceptions, individuals can better understand the responsibilities and requirements associated with the SSA-11 form and the role of a representative payee.
The SSA-11 form is used to request to be appointed as a representative payee for someone who is unable to manage their own Social Security benefits.
It is essential to provide accurate information about both the claimant and the payee. This includes names, Social Security numbers, and addresses.
Only fill out item 1 if you are the claimant requesting direct payment. If you are applying as a representative payee, skip to item 2.
Clearly explain why the claimant cannot handle their own benefits. This explanation should include details about how they manage any money they currently receive.
It is important to describe why you would be the best representative payee. Your qualifications and connection to the claimant can strengthen your application.
Indicate how you will stay informed about the claimant's needs. Regular visits or living arrangements can demonstrate your involvement.
If the claimant has a legal guardian or conservator, include their information. This helps the Social Security Administration understand the claimant's support system.
Be aware of the need to report any changes in the claimant's living situation or your own circumstances as a payee.
After submitting the form, you must use the benefits for the claimant's current needs or save them for future use.
Failure to comply with the responsibilities of a representative payee can lead to legal consequences, including the requirement to repay misused funds.