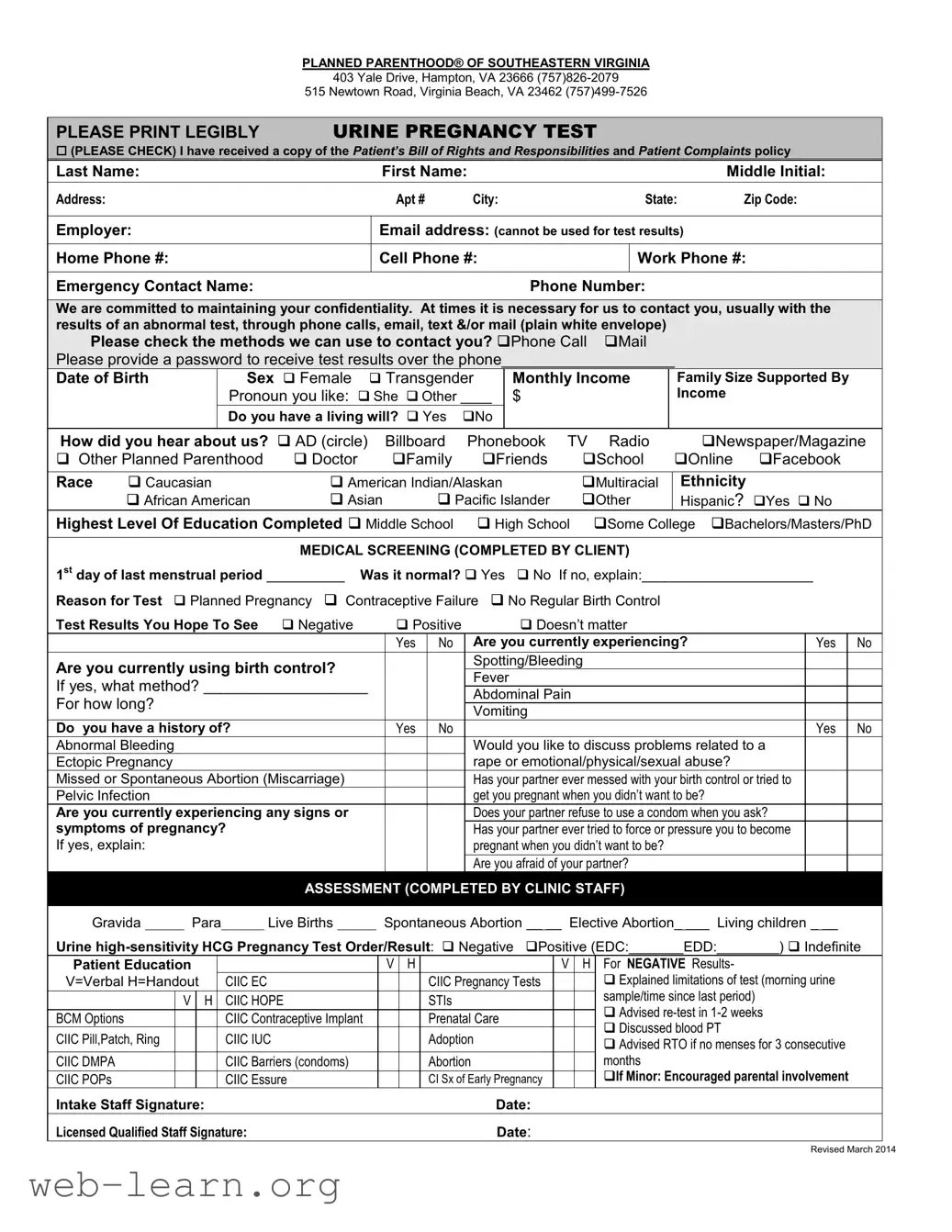
When seeking healthcare, especially related to reproductive health, clarity and understanding are paramount. The Planned Parenthood Proof form is an essential document that helps streamline the process for individuals seeking services at Planned Parenthood of Southeastern Virginia. This form collects vital information such as personal details, medical history, and contact preferences to ensure a tailored and confidential experience. Patients are prompted to check their preferred methods of communication for receiving test results, allowing for flexibility and comfort. Additionally, the form incorporates important sections covering medical screenings, including details about menstrual history and pregnancy symptoms. It also includes sections for assessing any potential risks related to interpersonal relationships, fostering a safe space for addressing sensitive topics. Overall, the Planned Parenthood Proof form serves not just as an administrative tool, but also as a first step in empowering individuals to take control of their health and well-being.

| Fact Name | Description |
|---|---|
| Provider Information | The form is from Planned Parenthood of Southeastern Virginia, with locations in Hampton and Virginia Beach. |
| Contact Methods | Patients can choose how they wish to be contacted regarding test results, including phone calls and mail. |
| Patient's Bill of Rights | Patients receive a copy of the Patient’s Bill of Rights and Responsibilities, ensuring they are aware of their rights in the healthcare setting. |
| Confidentiality Assurance | The form emphasizes the commitment to maintaining patient confidentiality through various communication methods. |
| State Compliance | This form aligns with Virginia state health care regulations, which require informed consent and confidentiality in medical practices. |
Completing the Planned Parenthood Proof form is an important step for those seeking medical services. It requires personal information, details about previous medical history, and consent for various communications. Your thoughtful approach to filling out this form helps ensure that your needs are understood and addressed effectively.
The Planned Parenthood Proof form is a document that patients fill out to access medical services at Planned Parenthood Southeastern Virginia. It includes personal information, medical history, and consent for treatment. This form helps ensure that the staff has necessary information for providing care, including details about pregnancy tests, contraception methods, and any pertinent medical conditions.
Confidentiality is a top priority at Planned Parenthood. Your personal and medical information will be kept private and handled according to health privacy laws. The form explicitly states that, while communication methods may include phone calls or mail, your contact methods will be limited to what you approve. Any sensitive information shared will be treated with the utmost discretion by the staff.
If you have questions or concerns while filling out the form, you are encouraged to speak with a clinic staff member. They are available to clarify any aspects of the form and ensure that you understand everything. It’s important to feel comfortable and informed about what you are consenting to, so don’t hesitate to ask for assistance.
While it is essential to provide accurate information for your care, you have the right to determine what personal details you disclose. However, some information may be critical for ensuring appropriate medical services. If you are uncomfortable providing certain details, it is best to discuss this with clinic staff, who can guide you on what is necessary for your treatment while respecting your privacy.
Filling out the Planned Parenthood Proof form can feel like a daunting task. It is essential to take your time and avoid common mistakes to ensure your information is accurate. One frequent error is inadequate legibility. If your handwriting is hard to read, it can lead to misunderstandings and delays. Always print clearly, as it is vital for your health care provider to have accurate contact information and personal details.
Another mistake is skipping sections of the form. Each part of the form serves a purpose. For instance, failing to complete the emergency contact information could hinder communication in a critical situation. Review the entire form before submitting, making sure that you haven't overlooked any required fields.
People also often forget to provide a password for test results via phone. This can slow down the process of receiving your results. Include a specific password so staff can verify your identity when they call.
Assuming that previous health information is still relevant can lead to incorrect assessments. Regularly update your medical history and ensure that you explicitly indicate any changes in your condition or treatments on the form.
Another common oversight is selecting the wrong methods of contact. Carefully consider how you would prefer to receive updates and results. Choosing a method that is inconvenient for you can create unnecessary stress, especially if urgent communication is needed.
Providing inaccurate information regarding household income could affect eligibility for financial assistance or services. It’s crucial to report this data as honestly as possible to avoid issues later on.
Additionally, misunderstanding questions about past medical history is common. Make sure you read each question thoroughly and respond accurately. Misrepresentation can lead to inappropriate treatment recommendations.
Lastly, neglecting to ask questions about anything unclear can leave you feeling uneasy about your care. If something on the form is confusing, don’t hesitate to ask staff for clarification. It’s better to have a complete understanding than to guess and potentially fill out the form incorrectly.
When visiting a Planned Parenthood facility, you may come across other important forms and documents in addition to the Planned Parenthood Proof form. These documents help ensure that your care is comprehensive and that your rights and privacy are respected. Here are some commonly used forms:
These forms are essential for a smooth experience at Planned Parenthood. They ensure that both you and the healthcare staff are on the same page regarding your care, rights, and privacy. Remember that asking questions and understanding these documents is always your right.
The Planned Parenthood Proof form shares similarities with several other documents related to healthcare and patient consent. Each of these documents serves a critical role in ensuring informed decision-making and the protection of patient rights.
When filling out the Planned Parenthood Proof form, ensuring accuracy and clarity is vital. Here are some key points to keep in mind:
This form is designed for anyone who may need reproductive health services, including transgender individuals and non-binary people. Gender-inclusive language is used to ensure everyone feels welcome and understood.
Signing the form simply gives consent for evaluation and education about available options. You can choose to opt-out of any services without any penalties.
Confidentiality is a top priority. The information provided is kept private and will only be shared in accordance with privacy laws or your explicit consent.
While the form requests an email address, it cannot be used for delivering test results. This is to protect your privacy. Other contact methods like phone or mail can be used instead.
You have the right to change your mind at any time regarding the services you choose to receive. Your autonomy and comfort are paramount.
A living will is optional. It is included on the form simply to gather information that may help in your care, but it is not a requirement for services.
Planned Parenthood Southeastern Virginia is a teaching institution. This means that trainees may assist in care under supervision. Nonetheless, licensed professionals ensure that you receive quality services.
Filling out the Planned Parenthood Proof form is an important step in ensuring you receive the medical services you need. Here are some key takeaways to help you navigate the process effectively:
By following these guidelines, you can help ensure that you complete the Planned Parenthood Proof form smoothly and receive the care needed for your health concerns.
Ct Realtors - A property condition report may be necessary, with potential credits to the buyer if not provided.
UB-04 Claim Form - The form allows for the entry of total charges and non-covered charges for transparency.
Hawaii Health Insurance Law - Do not use this form if you work for only one employer with coverage.