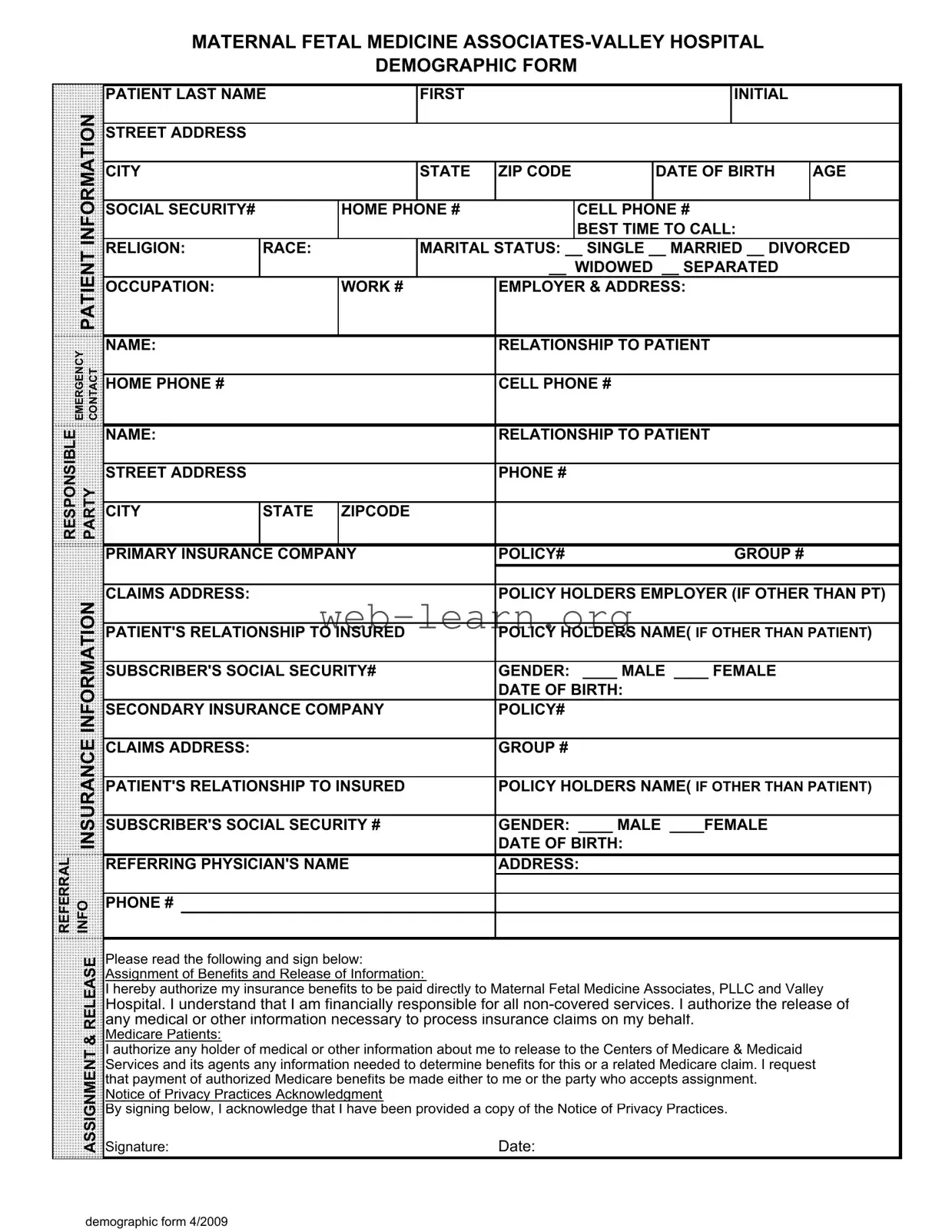
When visiting a healthcare provider, completing the Patient Demographics form is a vital step in ensuring that your medical care is tailored to your specific needs. This form collects essential information about you, including your name, address, date of birth, and contact details. It also asks about your insurance coverage, which is crucial for billing purposes. Additionally, the form gathers demographic details such as your marital status, occupation, and race, all of which can help healthcare providers better understand their patient population. Emergency contact information is requested to ensure that someone can be reached in case of unforeseen circumstances. Moreover, the form includes sections for both primary and secondary insurance information, which helps streamline the claims process. By signing the authorization for the release of information, you allow your healthcare provider to communicate with your insurance company, ensuring that your claims are processed efficiently. Understanding the importance of this form can enhance your healthcare experience and facilitate the administrative aspects of receiving care.
MATERNAL FETAL MEDICINE
DEMOGRAPHIC FORM
PATIENT LAST NAME |
FIRST |
INITIAL |
|
INFORMATION |
|
|
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
|
STATE |
ZIP CODE |
DATE OF BIRTH |
AGE |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
SOCIAL SECURITY# |
|
HOME PHONE # |
|
CELL PHONE # |
|
|||
|
|
|
|
|
|
|
|
BEST TIME TO CALL: |
|
|
|
PATIENT |
RELIGION: |
RACE: |
|
MARITAL STATUS: __ SINGLE __ MARRIED __ DIVORCED |
|||||
|
|
|
|
|
|
__ WIDOWED __ SEPARATED |
|
|||
|
|
|
|
|
|
|
|
|||
|
|
OCCUPATION: |
|
WORK # |
EMPLOYER & ADDRESS: |
|
||||
|
|
|
|
|
|
|
|
|
|
|
EMERGENCY CONTACT |
NAME: |
|
|
|
RELATIONSHIP TO PATIENT |
|
||||
|
|
|
|
|
|
|
|
|
||
HOME PHONE # |
|
|
|
CELL PHONE # |
|
|
||||
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
||
RESPONSIBLE |
|
NAME: |
|
|
|
RELATIONSHIP TO PATIENT |
|
|||
PARTY |
|
|
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
|
PHONE # |
|
|
||||
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
STATE |
ZIPCODE |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
PRIMARY INSURANCE COMPANY |
POLICY# |
GROUP # |
|
|||||
|
|
|
|
|
|
|
|
|||
|
INFORMATION |
CLAIMS ADDRESS: |
|
|
|
POLICY HOLDERS EMPLOYER (IF OTHER THAN PT) |
||||
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT'S RELATIONSHIP TO INSURED |
POLICY HOLDERS NAME( IF OTHER THAN PATIENT) |
||||||||
|
|
|||||||||
|
|
|
|
|
|
|||||
|
|
SUBSCRIBER'S SOCIAL SECURITY# |
GENDER: ____ MALE ____ FEMALE |
|
||||||
|
|
|
|
|
|
|
DATE OF BIRTH: |
|
|
|
|
|
SECONDARY INSURANCE COMPANY |
POLICY# |
|
|
|||||
|
INSURANCE |
|
|
|
|
|
|
|
|
|
|
CLAIMS ADDRESS: |
|
|
|
DATE OF BIRTH: |
|
|
|||
|
|
|
|
|
GROUP # |
|
|
|||
|
|
PATIENT'S RELATIONSHIP TO INSURED |
POLICY HOLDERS NAME( IF OTHER THAN PATIENT) |
|||||||
|
|
|
|
|
|
|||||
|
|
SUBSCRIBER'S SOCIAL SECURITY # |
GENDER: ____ MALE ____FEMALE |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
REFERRAL |
INFO |
REFERRING PHYSICIAN'S NAME |
ADDRESS: |
|
|
|||||
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
PHONE # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RELEASE |
Please read the following and sign below: |
|
|
|
|
||||
|
Assignment of Benefits and Release of Information: |
|
|
|
|
|||||
|
|
|
|
|
|
|||||
|
|
I hereby authorize my insurance benefits to be paid directly to Maternal Fetal Medicine Associates, PLLC and Valley |
||||||||
|
|
Hospital. I understand that I am financially responsible for all |
||||||||
|
|
any medical or other information necessary to process insurance claims on my behalf. |
|
|||||||
|
& |
Medicare Patients: |
|
|
|
|
|
|
|
|
|
I authorize any holder of medical or other information about me to release to the Centers of Medicare & Medicaid |
|
||||||||
|
ASSIGNMENT |
|
||||||||
|
Signature: |
|
|
|
Date: |
|
|
|||
|
|
Services and its agents any information needed to determine benefits for this or a related Medicare claim. I request |
||||||||
|
|
that payment of authorized Medicare benefits be made either to me or the party who accepts assignment. |
|
|||||||
|
|
Notice of Privacy Practices Acknowledgment |
|
|
|
|
||||
|
|
By signing below, I acknowledge that I have been provided a copy of the Notice of Privacy Practices. |
|
|||||||
demographic form 4/2009
| Fact Name | Details |
|---|---|
| Purpose | The Patient Demographics form collects essential information about patients to facilitate medical care and insurance processing. |
| Information Collected | It gathers personal details such as name, address, date of birth, contact numbers, and insurance information. |
| Emergency Contact | Patients must provide an emergency contact, including their relationship to the patient and contact numbers. |
| Insurance Details | The form requires information about primary and secondary insurance, including policy numbers and claims addresses. |
| Governing Law | In states like California, the form is governed by the California Confidentiality of Medical Information Act. |
| Patient Rights | Patients must acknowledge their rights regarding the release of medical information and assignment of benefits. |
| Privacy Acknowledgment | By signing, patients confirm they have received the Notice of Privacy Practices. |
| Demographic Updates | Patients should update their information regularly to ensure accuracy in medical records and billing. |
| Date of Form | This version of the demographic form was last updated in April 2009. |
Completing the Patient Demographics form is an essential step in ensuring that your medical information is accurately recorded. This form collects necessary details about you and your insurance coverage, which will help facilitate your care. Follow the steps below to fill out the form correctly.
What is the purpose of the Patient Demographics form?
The Patient Demographics form collects essential information about you to ensure accurate medical care and billing. This includes your personal details, insurance information, and emergency contacts. Providing this information helps the medical staff understand your needs better and streamline the process for your visits.
What information do I need to provide?
You will need to fill out various details, including:
Make sure all information is accurate to avoid delays in your care.
Why do you ask for my Social Security number?
Your Social Security number helps verify your identity and is often required by insurance companies for billing purposes. It is crucial for ensuring that your medical records are correctly associated with you.
What if I do not have insurance?
If you do not have insurance, you can still complete the form. Indicate that you are uninsured in the insurance section. The facility will provide information on payment options and financial assistance if needed.
How is my information protected?
Your information is kept confidential and is only used for medical and billing purposes. By signing the form, you acknowledge that you have received a copy of the Notice of Privacy Practices, which outlines how your information will be protected.
What should I do if my information changes?
If any of your information changes, such as your address, phone number, or insurance details, please notify the office as soon as possible. Keeping your information up to date is crucial for effective communication and billing.
Do I need to fill out this form for every visit?
Typically, you will not need to fill out the form for every visit unless there are significant changes in your information. However, it is a good practice to review your details at each appointment to ensure accuracy.
What happens if I don’t sign the release of information?
Signing the release of information is essential for processing your insurance claims. If you do not sign, it may delay your claims and could affect your ability to receive benefits. Ensure you read the release carefully before signing.
Filling out a Patient Demographics form can seem straightforward, but many individuals make common mistakes that can lead to complications later on. One frequent error is not providing complete information. For example, omitting the date of birth or leaving out the social security number can delay the processing of medical claims. Each piece of information is crucial for accurate record-keeping and insurance processing.
Another common mistake is using outdated information. Some patients may forget to update their address or phone number if they have recently moved. This can result in missed calls or important correspondence going to the wrong address. Keeping contact information current is essential for timely communication.
People often overlook the importance of accurately indicating their marital status. Whether someone is single, married, divorced, or widowed can affect insurance coverage and benefits. Misrepresenting this information can lead to misunderstandings and potential issues with claims.
Additionally, many individuals fail to specify their primary insurance company correctly. Providing the wrong policy number or group number can cause delays in claim processing. Always double-check these details to ensure they match what is listed on your insurance card.
Another mistake involves the emergency contact section. Some patients may not provide a reliable emergency contact or may list someone who is unavailable. It is crucial to choose someone who can be reached easily in case of an emergency.
Many people also forget to sign the release section of the form. This signature is necessary for the healthcare provider to process insurance claims on behalf of the patient. Without it, claims may be denied, leading to unexpected bills.
In addition, patients sometimes neglect to indicate their gender or provide the wrong information. This can lead to errors in medical records and affect treatment. It is important to be accurate in this section to ensure proper care.
Lastly, failing to read the Notice of Privacy Practices acknowledgment can lead to misunderstandings about how personal information is handled. Patients should take the time to understand their rights and the privacy policies of their healthcare providers. This knowledge can empower them and help prevent future issues.
The Patient Demographics form is a crucial document that gathers essential information about patients. It serves as the foundation for further administrative processes. In addition to this form, several other documents are commonly used to ensure comprehensive patient care and efficient management of medical records. Below is a list of these documents.
These forms work together with the Patient Demographics form to create a complete picture of the patient's health and administrative needs. Proper completion and management of these documents facilitate effective communication and care within the healthcare system.
The Patient Demographics form serves as a vital document in healthcare settings, collecting essential information about patients. Several other documents share similarities with this form in terms of the type of information gathered and their purpose. Below is a list of eight such documents:
When filling out the Patient Demographics form, it's important to be careful and thorough. Here are some dos and don'ts to keep in mind:
Understanding the Patient Demographics form is essential for both patients and healthcare providers. However, several misconceptions can lead to confusion. Here are seven common misunderstandings:
By addressing these misconceptions, patients can better understand the importance of the Patient Demographics form and how it contributes to their healthcare experience.
Completing the Patient Demographics form accurately is essential for ensuring proper care and communication. Here are key takeaways to keep in mind:
By following these guidelines, you can help ensure that your experience is smooth and that your healthcare providers have the necessary information to assist you effectively.