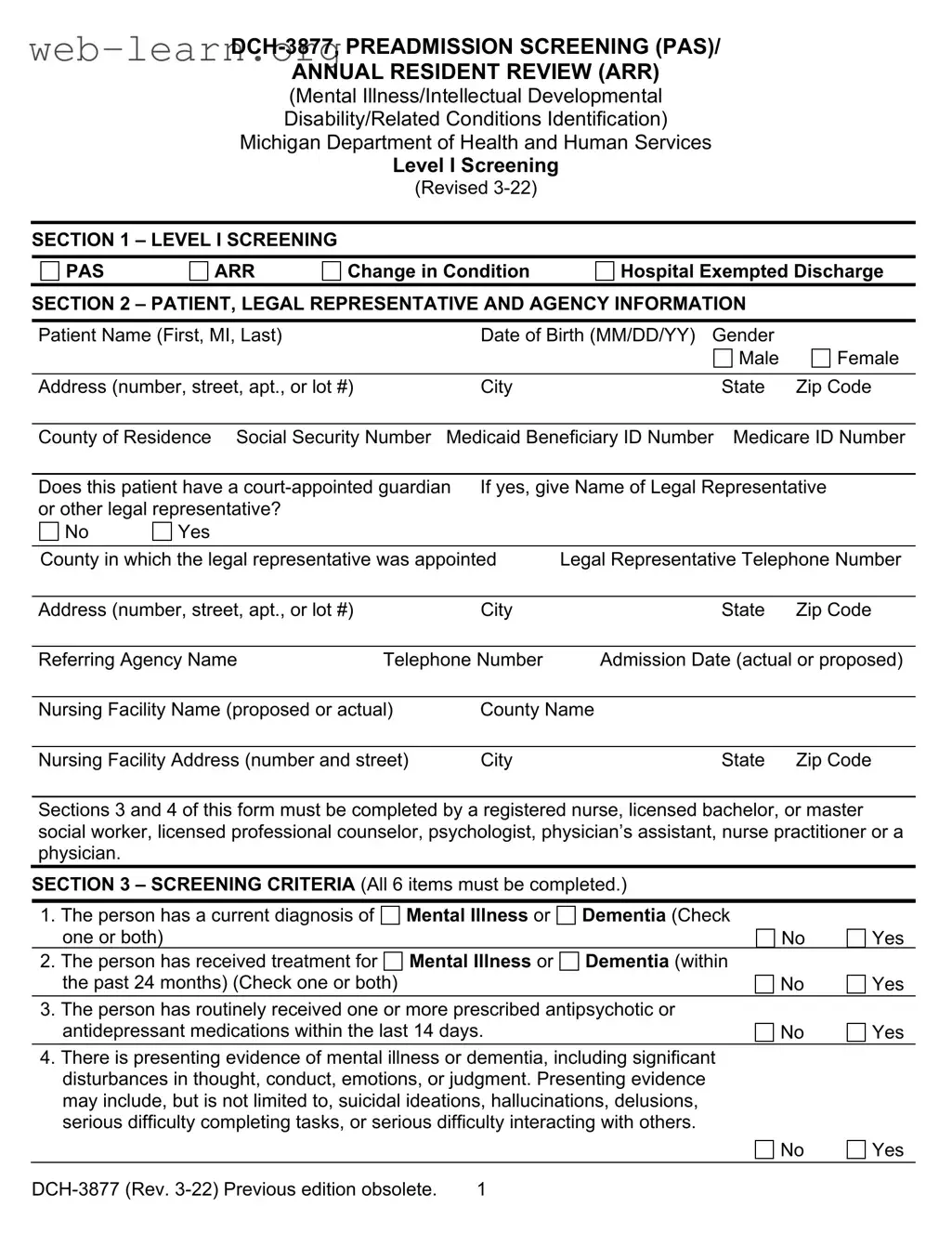
The Michigan DCH 3877 form plays a crucial role in the evaluation and admission process for individuals seeking services in nursing facilities, particularly those with potential mental health concerns or developmental disabilities. This form, officially known as the Preadmission Screening (PAS) and Annual Resident Review (ARR), is designed to identify whether a prospective or current resident meets specific criteria for mental illness or developmental disabilities. It requires completion by qualified professionals, such as registered nurses or physicians, ensuring that the assessment is thorough and accurate. Among its key components are questions that help determine if an individual has a current diagnosis of mental illness or dementia, has received relevant treatment in the past two years, or shows signs of developmental disabilities. The form also emphasizes the importance of documenting patient information, including personal details and the involvement of any legal guardians. Additionally, the DCH 3877 is closely linked to another form, the DCH 3878, which addresses exemption criteria for certain cases. Understanding the nuances of the DCH 3877 form is essential for healthcare providers, as it directly impacts the eligibility for Medicaid services and the overall care that individuals receive in nursing facilities.
ANNUAL RESIDENT REVIEW (ARR)
(Mental Illness/Intellectual Developmental
Disability/Related Conditions Identification)
Michigan Department of Health and Human Services
Level I Screening
(Revised
SECTION 1 – LEVEL I SCREENING
PAS |
|
ARR |
Change in Condition |
Hospital Exempted Discharge |
||
SECTION 2 – PATIENT, LEGAL REPRESENTATIVE AND AGENCY INFORMATION |
|
|||||
Patient Name (First, MI, Last) |
|
Date of Birth (MM/DD/YY) Gender |
|
|||
|
|
|
|
|
Male |
Female |
Address (number, street, apt., or lot #) |
City |
State |
Zip Code |
|||
|
|
|||||
County of Residence |
Social Security Number Medicaid Beneficiary ID Number Medicare ID Number |
|||||
|
|
|||||
Does this patient have a |
If yes, give Name of Legal Representative |
|||||
or other legal representative? |
|
|
|
|
||
No |
Yes |
|
|
|
|
|
County in which the legal representative was appointed |
Legal Representative Telephone Number |
|||||
|
|
|
|
|||
Address (number, street, apt., or lot #) |
City |
State |
Zip Code |
|||
|
|
|
||||
Referring Agency Name |
Telephone Number |
Admission Date (actual or proposed) |
||||
|
|
|
||||
Nursing Facility Name (proposed or actual) |
County Name |
|
||||
|
|
|
|
|||
Nursing Facility Address (number and street) |
City |
State |
Zip Code |
|||
Sections 3 and 4 of this form must be completed by a registered nurse, licensed bachelor, or master social worker, licensed professional counselor, psychologist, physician’s assistant, nurse practitioner or a physician.
SECTION 3 – SCREENING CRITERIA (All 6 items must be completed.)
1. |
The person has a current diagnosis of |
Mental Illness or |
Dementia (Check |
|
|
||
|
one or both) |
|
|
|
No |
|
Yes |
|
|
|
|
|
|||
2. |
The person has received treatment for |
Mental Illness or |
Dementia (within |
|
|
|
|
|
the past 24 months) (Check one or both) |
|
|
|
No |
|
Yes |
3. |
The person has routinely received one or more prescribed antipsychotic or |
|
|
||||
|
antidepressant medications within the last 14 days. |
|
|
No |
|
Yes |
|
4.There is presenting evidence of mental illness or dementia, including significant disturbances in thought, conduct, emotions, or judgment. Presenting evidence may include, but is not limited to, suicidal ideations, hallucinations, delusions, serious difficulty completing tasks, or serious difficulty interacting with others.
No |
Yes |
1 |
5.The person has a diagnosis of an intellectual/developmental disability or a related condition including, but not limited to, epilepsy, autism, or cerebral palsy and this
diagnosis manifested before the age of 22. |
No |
Yes |
6.There is presenting evidence of deficits in intellectual functioning or adaptive behavior which suggests that the person may have an intellectual/developmental disability or a related condition. These deficits appear to have manifested before
the age of 22. |
No |
Yes |
Note: If you checked “Yes” to items 1 and/or 2, checked the word “Mental Illness” and/or “Dementia.”
If yes, please explain
Note: The person screened shall be determined to require a comprehensive Level II OBRA evaluation if any of the above items are "Yes" UNLESS a physician, nurse practitioner or physician’s assistant certifies on form
SECTION 4 - CLINICIAN’S STATEMENT: I certify to the best of my knowledge that the above information is accurate.
Clinician Signature |
Date |
Name (type or print) |
|
|
|
Degree/License |
|
Telephone Number |
|
|
|
The Michigan Department of Health and Human Services will not exclude from participation in, deny benefits of, or discriminate against any individual or group because of race, sex, religion, age, national origin, color, height, weight, marital status, partisan considerations, or a disability or genetic information that is unrelated to the person’s eligibility.
AUTHORITY: Title XIX of the Social Security Act
COMPLETION: Is voluntary, however, if NOT completed, Medicaid will not reimburse the nursing facility.
DISTRIBUTION: If any answer to items 1 – 6 in SECTION 3 is "Yes", send ONE copy to the local Community Mental Health Services Program (CMHSP), with a copy of form
2 |
PREADMISSION SCREENING (PAS)/ANNUAL RESIDENT REVIEW (ARR)
Mental Illness/Intellectual Developmental Disability/Related Conditions Identification
Instructions for Completing Level I Screening
This form is used to identify prospective and current nursing facility residents who meet the criteria for possible mental illness or intellectual/developmental disability, or a related condition and who may be in need of mental health services.
Sections II and III must be completed by a registered nurse, licensed bachelor, or master social worker, licensed professional counselor, psychologist, physician’s assistant, nurse practitioner or physician.
Preadmission Screening or Hospital Exempted Discharge: The referral source completing the Level I Screening
Annual Resident Review or Change in Condition: This form must be completed by the nursing facility.
Check the appropriate box in the upper
Section II – Screening Criteria – All 6 items in this section must be completed. The following provides additional explanation of the items.
1.Mental Illness: A current primary diagnosis of a mental disorder as defined in the American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders.
Current Diagnosis means that a clinician has established a diagnosis of a mental disorder within the past 24 months. Do NOT mark “Yes” for an individual cited as having a diagnosis "by history" only.
2.Receipt of treatment for mental illness or dementia within the past 24 months means any of the following: inpatient psychiatric hospitalization; outpatient services such as psychotherapy, day program, or mental health case management; or referral for psychiatric consultation, evaluation, or prescription of psychopharmacological medications.
3.Antidepressant and antipsychotic medications mean any currently prescribed medication classified as an antidepressant or antipsychotic, plus Lithium Carbonate and Lithium Citrate.
4.Presenting evidence means the individual currently manifests symptoms of mental illness or dementia, which suggests the need for further evaluation to establish causal factors, diagnosis, and treatment recommendations. Further evaluation may need to be completed if evidence of suicidal ideation, hallucinations, delusion, serious difficulty completing tasks or serious difficulty interacting with others.
5.Intellectual/Developmental Disability/Related Condition: An individual is considered to have a severe, chronic disability that meets ALL 4 of the following conditions:
a.It is manifested before the person reaches age 22.
b.It is likely to continue indefinitely.
c.It results in substantial functional limitations in 3 or more of the following areas of major life activity:
d.It is attributable to:
•Intellectual/Developmental Disability such that the person has significant subaverage general intellectual functioning existing concurrently with deficits in adaptive behavior and manifested during the developmental period;
•cerebral palsy, epilepsy, autism; or
3 |
•any condition other than mental illness found to be closely related to Intellectual/ Developmental Disability because this condition results in impairment in general intellectual functioning OR adaptive behavior similar to that of persons with Intellectual/Developmental Disability and requires treatment or services similar to those required for these persons.
6.Presenting evidence means the individual manifests deficits in intellectual functioning or adaptive behavior, which suggests the need for further evaluation to determine the presence of a developmental disability, causal factors, and treatment recommendations. These deficits appear to have manifested before the age of 22.
Note: When there are one or more "Yes" answers to items 1 – 6 under SECTION II, complete form
4 |
| Fact Name | Details |
|---|---|
| Form Purpose | The DCH-3877 is used to identify individuals in nursing facilities who may have mental illness or developmental disabilities. |
| Governing Law | The form is governed by P.A. 280 of 1939 and Title XIX of the Social Security Act. |
| Issuance Date | The DCH-3877 was issued on July 1, 2003. |
| Distribution | This form is distributed to nursing facilities, hospitals, and community mental health service programs. |
| Completion Requirements | A registered nurse, social worker, psychologist, physician’s assistant, or physician must complete the form. |
| Screening Criteria | Six specific criteria must be answered to determine the need for further evaluation. |
| Form Updates | The DCH-3877 replaced the obsolete MSA-3877 form, reflecting updated diagnostic criteria. |
| Exemption Criteria | Physicians can certify exemptions for patients under certain conditions, including dementia or coma. |
| Ordering Information | Forms can be ordered from the Michigan Department of Community Health or downloaded from their website. |
| Contact Information | Providers can reach out to Provider Inquiry at the Department of Community Health for any questions. |
Filling out the Michigan DCH-3877 form requires careful attention to detail. This form is essential for assessing individuals who may need mental health services as part of their admission to a nursing facility. Follow the steps below to ensure accurate completion of the form.
Once the form is completed and distributed as outlined, it will be ready for the necessary processing. Ensure that all information is accurate to avoid delays in the patient's admission and care. If there are any questions during the process, contact the Department of Community Health for assistance.
What is the purpose of the Michigan DCH-3877 form?
The Michigan DCH-3877 form is designed to identify prospective and current nursing facility residents who may have mental illness or developmental disabilities. This identification is crucial for determining whether individuals require mental health services. The form must be completed by qualified professionals, such as registered nurses, social workers, psychologists, or physicians, as part of the preadmission screening or annual resident review processes.
Who is responsible for completing the DCH-3877 form?
The completion of the DCH-3877 form is the responsibility of a registered nurse, certified or registered social worker, psychologist, physician’s assistant, or physician. These professionals must ensure that all required sections of the form are accurately filled out, particularly the screening criteria that assess the presence of mental illness or developmental disabilities.
What changes were made to the DCH-3877 form in the latest revision?
The most recent revision of the DCH-3877 form included several important updates. The form now reflects its designation as a Department of Community Health (DCH) form. Additionally, the terminology has been updated, changing "exception" to "exemption" and revising the references to mental health classifications. The changes also include updates to the criteria for dementia diagnoses and the addition of provisions for other primary psychiatric diagnoses.
How can providers obtain the DCH-3877 form?
Providers can obtain the DCH-3877 form by ordering it directly from the Michigan Department of Community Health, specifically from the Forms Distribution office located in Lansing, Michigan. Alternatively, the form is available for download from the Michigan Department of Community Health website. By navigating to the appropriate section for Medicaid provider forms, providers can easily access and print the necessary documents.
Filling out the Michigan DCH-3877 form can be a daunting task, especially for those unfamiliar with its requirements. One common mistake is failing to provide complete patient information. It’s essential to ensure that all fields, such as the patient's name, date of birth, and address, are filled out accurately. Missing or incorrect information can lead to delays in processing and may even affect the eligibility for services.
Another frequent error involves not understanding the screening criteria outlined in Section II. Many people overlook the importance of circling the appropriate diagnosis, whether it’s “mental illness” or “dementia,” when answering questions one and two. This step is crucial, as it directly influences whether the individual will require further evaluation. Skipping this detail can result in unnecessary complications.
Many individuals also struggle with the requirement that certain professionals complete the form. Only registered nurses, certified social workers, psychologists, physician assistants, or physicians are authorized to fill out Sections II and III. If someone without the proper credentials attempts to complete these sections, it can invalidate the form, leading to rejection of the application.
In addition, people often misinterpret the meaning of “presenting evidence” in the screening criteria. It's not enough to simply check “yes” to questions three through six; the form requires a detailed explanation of any “yes” answers. Providing vague or insufficient explanations can hinder the review process and may result in further requests for information.
Another common oversight is neglecting to check the correct box for either Preadmission Screening (PAS) or Annual Resident Review (ARR). This distinction is important as it determines the context in which the form is being submitted. Failing to make this selection can lead to confusion and delays in processing.
Lastly, individuals often forget to retain copies of the completed form for their records. Keeping a copy is crucial for tracking the submission and ensuring that all necessary follow-up actions are taken. Without this documentation, it may be challenging to resolve any issues that arise later in the process.
The Michigan DCH-3877 form is an essential document used in the process of evaluating individuals for mental illness or developmental disabilities prior to admission to nursing facilities. This form is often accompanied by several other important documents that help streamline the assessment and ensure that all necessary information is collected. Below is a list of forms commonly used alongside the DCH-3877, each serving a specific purpose in the evaluation process.
Each of these documents plays a vital role in the comprehensive evaluation and care of individuals seeking assistance in nursing facilities. By ensuring that all necessary forms are completed accurately and promptly, healthcare providers can facilitate a smoother admission process and better address the needs of their patients.
The Michigan DCH-3877 form is part of a crucial process for assessing individuals who may require mental health services. It shares similarities with several other documents that serve similar purposes in the healthcare and social services sectors. Below is a list of ten documents that are comparable to the DCH-3877, along with explanations of their similarities:
Understanding these similarities is essential for ensuring that individuals receive the necessary evaluations and services. Each document plays a vital role in the continuum of care, making it imperative for providers to be familiar with them.
When filling out the Michigan DCH-3877 form, it is essential to follow certain guidelines to ensure accuracy and compliance. Here are six things you should and shouldn’t do:
Understanding the Michigan DCH-3877 form is essential for healthcare providers and patients alike. However, several misconceptions exist regarding its purpose and requirements. Below are nine common misconceptions, along with clarifications for each.
Addressing these misconceptions can help ensure that patients receive the necessary evaluations and services while complying with Medicaid requirements. Understanding the nuances of the DCH-3877 form is crucial for effective patient care.
The Michigan DCH-3877 form is essential for identifying individuals who may require mental health services as part of the Preadmission Screening and Annual Resident Review processes. Here are key takeaways regarding its completion and use:
Understanding these points ensures accurate and effective use of the DCH-3877 form in the healthcare process.