In the realm of healthcare, maintaining accurate records is essential for ensuring patient safety and effective medication management. One critical tool in this process is the Medication Count Sheet form. This form serves as a comprehensive log, meticulously tracking the administration of medications to residents. It includes vital information such as the resident's name, the quantity of medication prescribed, and the date the medication regimen was initiated. Each entry also captures the drug's strength, providing clarity on the dosage being administered. Staff members play a crucial role in this documentation, as their signatures confirm the accuracy of the records. The form includes sections for recording the date and time of administration, allowing for precise monitoring of medication schedules. Additionally, it facilitates a count of the quantities on hand, those administered, and what remains, ensuring that discrepancies can be swiftly identified and addressed. By utilizing the Medication Count Sheet, healthcare providers can enhance their accountability and uphold the highest standards of care for their patients.
|
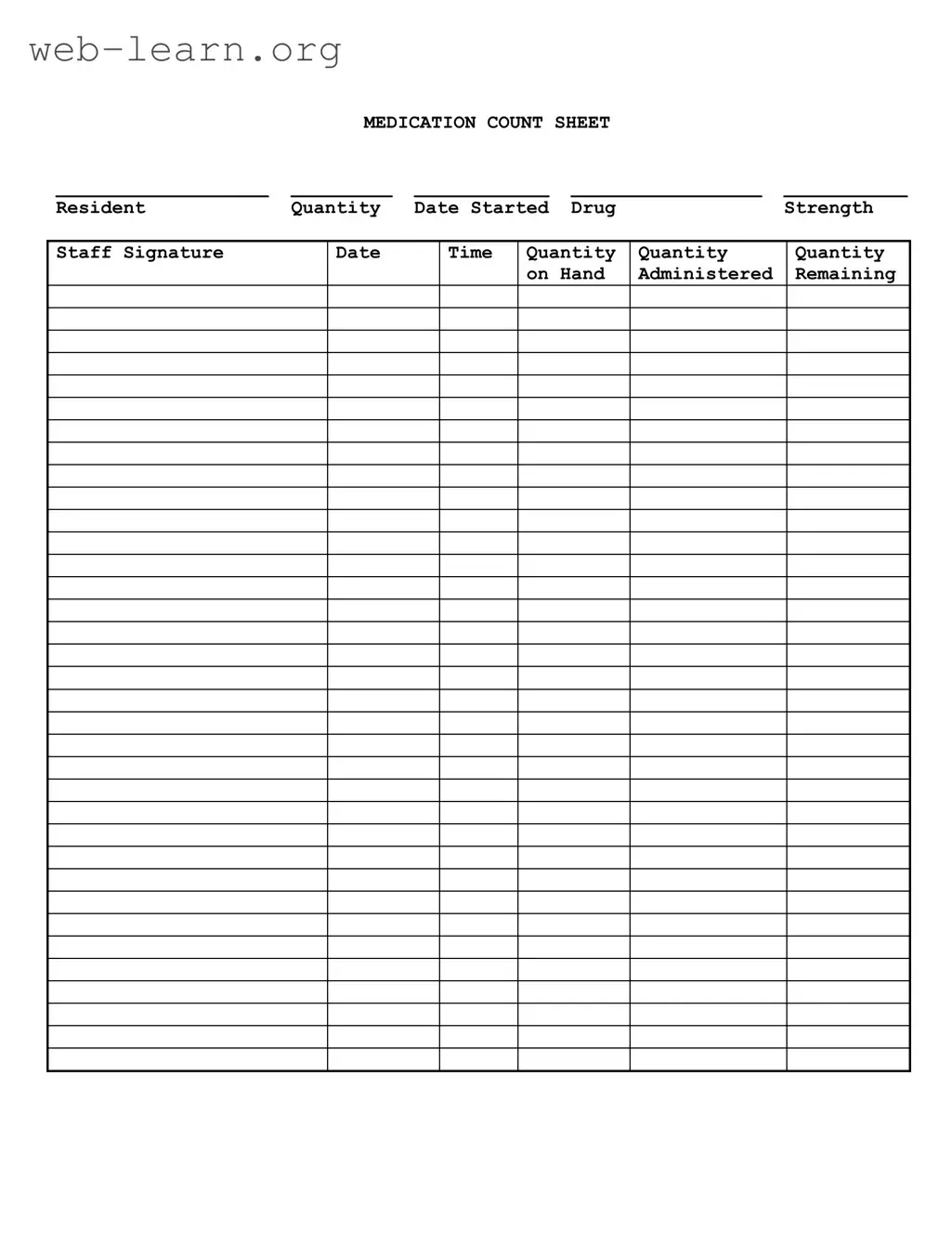
MEDICATION COUNT SHEET |
|
||
___________________ |
_________ |
____________ |
_________________ |
___________ |
Resident |
Quantity |
Date Started |
Drug |
Strength |
Staff Signature
Date
Time
Quantity |
Quantity |
Quantity |
on Hand |
Administered |
Remaining |
|
|
|
| Fact Name | Description |
|---|---|
| Purpose | The Medication Count Sheet is used to track the administration and inventory of medications for residents. |
| Required Information | Essential details include resident name, drug strength, quantity administered, and remaining quantity on hand. |
| Staff Accountability | Staff members must sign the sheet to confirm medication administration, ensuring accountability and traceability. |
| Frequency of Use | This form should be updated each time medication is administered or a new supply is received. |
| State-Specific Regulations | In California, the governing law is Title 22, Section 87505, which mandates accurate medication records. |
| Importance of Accuracy | Accurate record-keeping is crucial for patient safety and compliance with healthcare regulations. |
After completing the Medication Count Sheet form, you will have a clear record of the medication inventory for the resident. This ensures accountability and helps maintain accurate medication management. Follow the steps below to fill out the form correctly.
The Medication Count Sheet is designed to track the administration and inventory of medications for residents. It helps ensure that medications are given correctly and that there is an accurate record of what is on hand.
The form includes several key pieces of information:
Staff members who administer medications are responsible for completing the Medication Count Sheet. They must ensure that all sections are filled out accurately to maintain proper records.
The Medication Count Sheet should be updated each time medication is administered. This ensures that the quantity on hand reflects the most current information and helps prevent errors.
If a discrepancy is found, staff should immediately investigate the issue. This may involve checking records, recounting medications, and discussing with other staff members. It is important to resolve discrepancies promptly to ensure the safety of residents.
Filling out the Medication Count Sheet form accurately is crucial for ensuring proper medication management. However, many individuals make common mistakes that can lead to serious issues. One frequent error is failing to record the date clearly. Without a precise date, tracking medication administration becomes challenging. It can lead to confusion about when a medication was started or administered, which is vital for maintaining the health and safety of residents.
Another mistake often seen is neglecting to update the quantity on hand after administering medication. This oversight can result in discrepancies in the medication count. If the amount remaining is not adjusted, staff may mistakenly believe there is more medication available than there actually is. This could lead to medication shortages or overdoses, both of which pose significant risks to patient safety.
Additionally, some staff members forget to include their signature on the form. The signature serves as a verification that the medication was administered as recorded. Without it, there is no accountability, and it can become difficult to trace who was responsible for the medication administration. This lack of accountability can have serious implications during audits or investigations.
Lastly, people often skip filling out the time of administration. Recording the time is essential for monitoring medication schedules. If the time is left blank, it can lead to confusion about when the last dose was given. This is particularly important for medications that need to be administered at specific intervals. Accurate time recording helps ensure that residents receive their medications safely and on schedule.
The Medication Count Sheet is a crucial tool for tracking medication administration and inventory in healthcare settings. However, it is often accompanied by several other forms and documents that help ensure accurate record-keeping and compliance with regulations. Here’s a brief overview of some of these documents.
Utilizing these forms alongside the Medication Count Sheet enhances accountability and ensures a high standard of care. Accurate documentation is essential in maintaining the integrity of medication management systems in healthcare facilities.
The Medication Count Sheet form is an essential tool in healthcare settings, particularly in managing and tracking medication administration. Several other documents serve similar purposes in ensuring accurate medication management. Here are four such documents:
When filling out the Medication Count Sheet form, attention to detail is crucial. Here are some important dos and don'ts to keep in mind:
Understanding the Medication Count Sheet form is crucial for ensuring proper medication management. However, several misconceptions can lead to confusion. Here’s a list of ten common misunderstandings about this important document.
By addressing these misconceptions, individuals can better understand the Medication Count Sheet form and its vital role in medication management. Accurate documentation promotes safety and accountability in healthcare settings.
When using the Medication Count Sheet form, it is essential to follow specific guidelines to ensure accuracy and compliance. Here are some key takeaways: