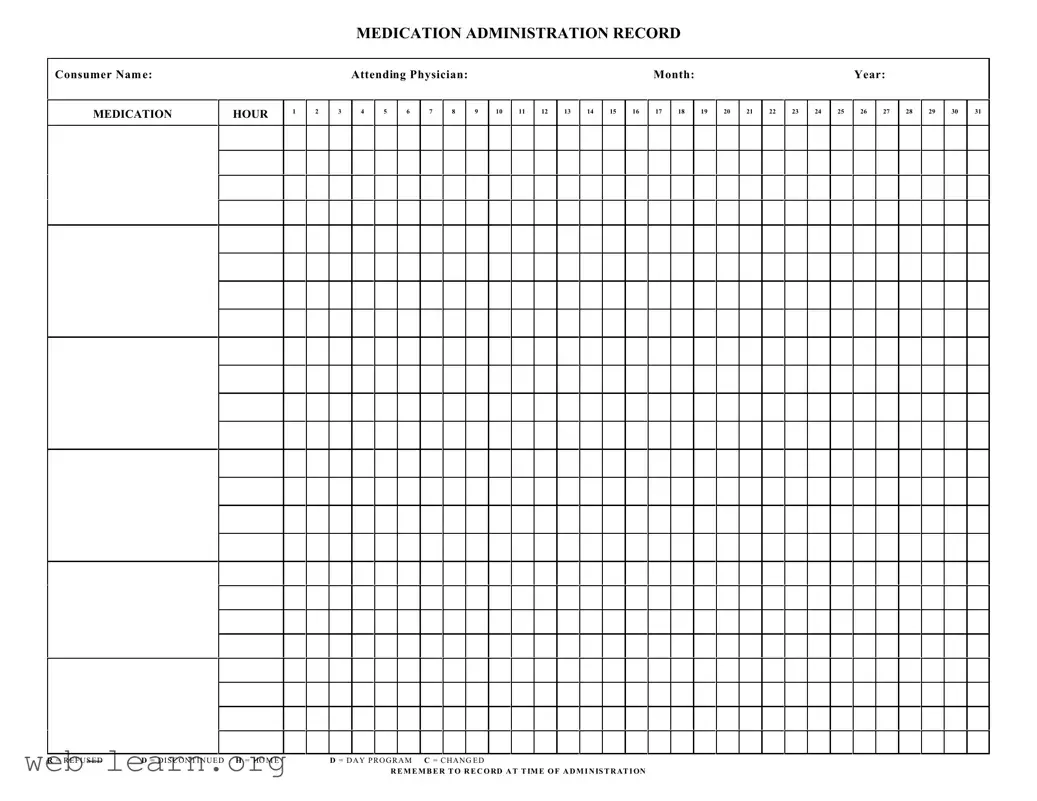
The Medication Administration Record Sheet is an essential tool in healthcare settings, particularly for ensuring the safe and effective administration of medications to patients. This form captures vital information, including the consumer's name, attending physician, and relevant dates, allowing healthcare professionals to track each medication administered throughout the month. Organized into a grid format, the form includes designated hours for medication intake, noted by numbered columns that facilitate easy reference. Each day features specific designations, such as 'R' for refused, 'D' for discontinued, 'H' for home, and 'C' for changed, to ensure clarity in medication management. It serves not only as a record of what has been administered but also as a prompt for healthcare providers to document thoroughly. Proper usage of this form is critical; it requires diligent recording at the time of administration to maintain accurate medication histories and avoid potential errors. By following the established protocols outlined in the form, caregivers can enhance the quality of care while providing a reliable reference for ongoing treatment decisions.
| Fact Name | Description |
|---|---|
| Purpose | The Medication Administration Record Sheet is used to document medication administration for consumers. |
| Consumer Information | It includes fields for the consumer's name and identifies the attending physician. |
| Date Tracking | The form must reflect the month and year of the medication administration. |
| Hourly Documentation | It provides designated hours (1-31) to record each dose of medication taken. |
| Refusal Indicator | The form allows noting if a medication was refused with an "R" for refused. |
| Discontinued Indicator | An "D" is used to indicate if a medication has been discontinued. |
| Home and Day Program Codes | Initials "H" and "D" indicate whether the medication is administered at home or through a day program. |
| Change Indicator | Medications that have been changed are marked with a "C". |
| Record Timing | It is critical to record information at the time of administration for accuracy. |
| State Regulation | Each state may have specific laws governing the use of Medication Administration Records. For example, in California, it is guided by Health and Safety Code § 1250.3. |
Completing the Medication Administration Record Sheet accurately is important to ensure proper documentation of medication given to individuals. Follow these steps carefully to fill out the form correctly.
Careful attention to each of these steps helps maintain high standards in medication management. Your diligence ensures that those under your care receive the right treatments safely and effectively.
What is a Medication Administration Record (MAR) sheet?
A Medication Administration Record sheet is a form used to track and document the administration of medications to a patient or consumer. It helps ensure that medications are given as prescribed and assists healthcare providers in monitoring the patient's response to treatments.
Who should use the MAR sheet?
The MAR sheet is primarily used by healthcare professionals, such as nurses and caregivers, who administer medications. It can also be helpful for family members or guardians overseeing a loved one's medication regimen.
What information is included in the MAR sheet?
The MAR sheet typically includes:
How do I properly fill out the MAR sheet?
To fill out the MAR sheet, follow these steps:
Why is it important to keep an accurate MAR sheet?
Maintaining an accurate MAR sheet is critical for several reasons. It helps prevent medication errors, ensures adherence to prescribed treatment plans, and provides a clear record of what was given to the consumer. This documentation can become vital in case of emergencies or when assessing the effectiveness of the treatment.
What should I do if there is a mistake on the MAR sheet?
If you notice a mistake, such as an incorrect entry, it’s essential to correct it promptly. Cross out the error neatly, initial it, and enter the correct information. Avoid using correction fluid, as it can obscure vital information. Always ensure the correction is clear and does not mislead anyone reviewing the document.
Completing the Medication Administration Record Sheet is crucial for ensuring proper medication management. One common mistake is failing to include the consumer's full name. An incomplete name can lead to confusion, especially in facilities with multiple consumers. Always verify that the name matches the prescription to avoid errors.
Another frequent error involves neglecting to document the time of administration. This step is vital for tracking whether medications are given on schedule. Omitting this information might result in missed doses or potential overdoses. Be diligent about recording the exact time when each medication is administered.
Sometimes, individuals mistakenly mark the wrong column for dosage. Each hour must be clearly indicated to avoid miscommunication among staff members. Each dose, including any refusals or changes, should be carefully logged to keep all caregivers informed and ensure compliance with prescribed treatment.
Using abbreviations incorrectly can also lead to serious misunderstandings. For example, some may confuse "D" for "Discontinued" with "D" for "Day Program." Properly defining abbreviations used on the record sheet is paramount to maintaining clarity in communication. Every member of the healthcare team should know what each symbol stands for.
Finally, failing to double-check entries before submission is a significant oversight. Simple mistakes can have serious repercussions. Always take a moment to review the entire record for accuracy. This not only ensures the safety of the consumer but also helps maintain professionalism within the caregiving environment.
When managing medication for consumers, various forms and documents play a crucial role in ensuring safety and compliance. Below is a list of common documents frequently used alongside the Medication Administration Record Sheet form. Each document serves a specific purpose and adds to the overall understanding and management of medication administration.
These documents are essential for a thorough and effective medication administration process. Each one contributes to a comprehensive understanding of the consumer's medication needs, promoting safety and well-being.
When filling out the Medication Administration Record Sheet form, there are important guidelines to follow to ensure the process is accurate and effective. Here are seven things to do and avoid:
Misconceptions about the Medication Administration Record Sheet can lead to confusion and errors in medication management. Here are eight common misconceptions:
When using the Medication Administration Record Sheet form, consider these important points:
Comptroller Nyc - Claimants can track the status of their claims through the NYC Comptroller's website.
Notice of Change of Address - Parties involved in the case must be kept informed of any changes to their representation status.