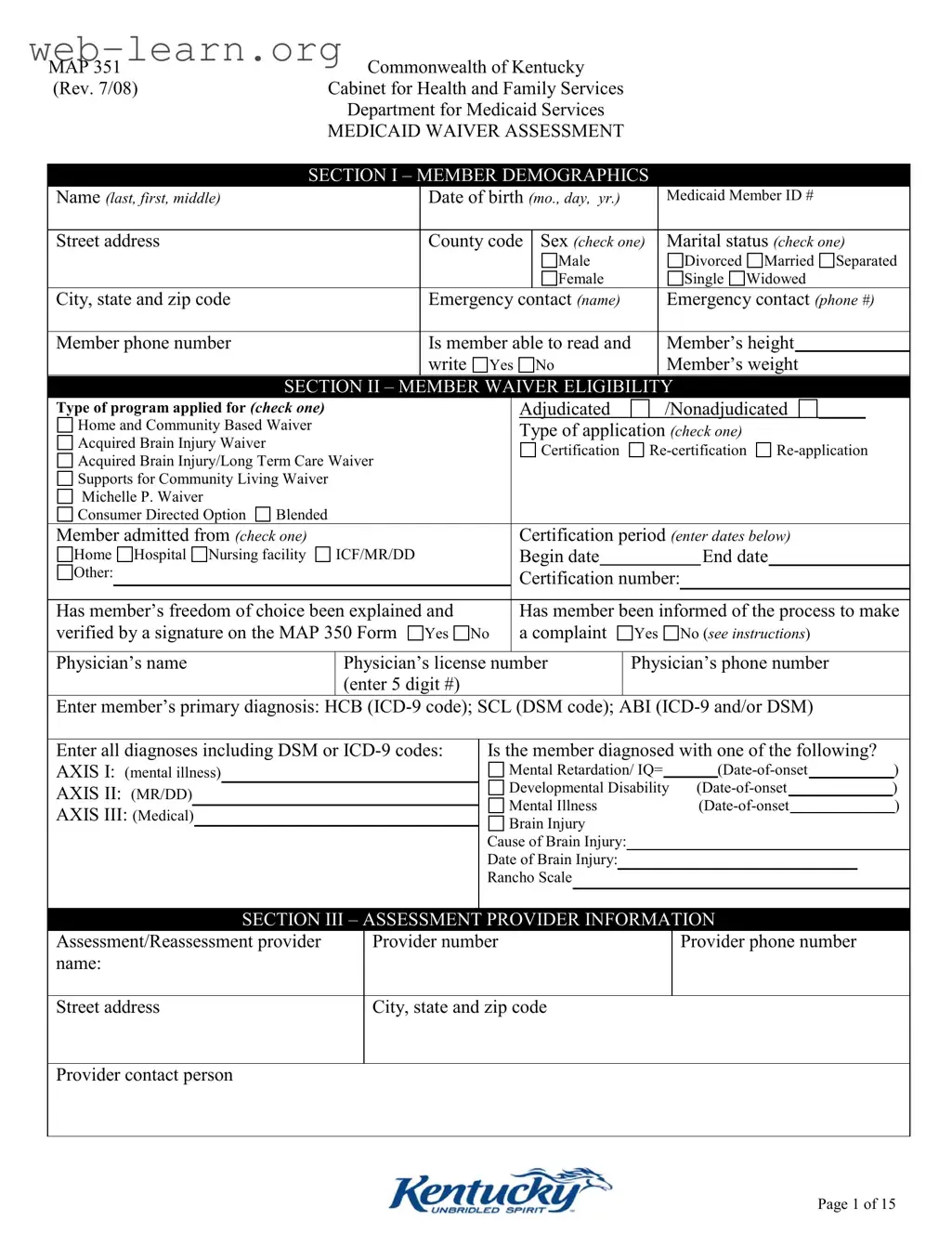
The Kentucky Map 351 form serves as a critical tool in the Medicaid Waiver assessment process, designed to gather essential information about individuals seeking access to various waiver programs. This comprehensive document encompasses several sections that detail member demographics, eligibility criteria, and assessment of daily living activities. The first section collects basic personal information, including the member's name, date of birth, and Medicaid ID, along with emergency contact details. Following this, the form delves into the specific waiver eligibility, allowing applicants to indicate the type of program they are applying for, such as Home and Community-Based Waivers or the Acquired Brain Injury Waiver. The assessment also addresses the member’s abilities in daily activities, ranging from personal care tasks like dressing and grooming to instrumental activities such as meal preparation and managing finances. Furthermore, the form includes a section dedicated to neuro/emotional and behavioral assessments, ensuring a holistic view of the member’s needs and challenges. By meticulously documenting this information, the Kentucky Map 351 form plays a vital role in determining the appropriate level of support and services for individuals with varying needs, ultimately facilitating their access to essential resources.
MAP 351 |
Commonwealth of Kentucky |
|
|
|
|
|
|
|
|
|
|
|
||||||||
(Rev. 7/08) |
Cabinet for Health and Family Services |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
Department for Medicaid Services |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
MEDICAID WAIVER ASSESSMENT |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
SECTION I – MEMBER DEMOGRAPHICS |
|
|
|
|
|
|
|
|
|
|||||||||
|
Name (last, first, middle) |
|
Date of birth (mo., day, yr.) |
|
|
Medicaid Member ID # |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Street address |
|
County code |
Sex (check one) |
Marital status (check one) |
|||||||||||||||
|
|
|
|
|
|
|
|
Male |
|
|
|
Divorced |
Married |
Separated |
||||||
|
|
|
|
|
|
|
|
Female |
|
|
|
Single |
Widowed |
|
|
|||||
|
City, state and zip code |
|
Emergency contact (name) |
|
|
Emergency contact (phone #) |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Member phone number |
|
Is member able to read and |
Member’s height |
|
|
||||||||||||||
|
|
|
|
write |
Yes |
|
No |
|
|
Member’s weight |
|
|
|
|||||||
|
|
SECTION II – MEMBER WAIVER ELIGIBILITY |
|
|
|
|
|
|
||||||||||||
|
Type of program applied for (CHECK ONE) |
|
|
|
|
Adjudicated |
|
|
/Nonadjudicated |
|
_____ |
|
||||||||
|
|
|
|
|
|
|
|
|||||||||||||
|
Home and Community Based Waiver |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
Type of application (check one) |
|
|
|
|
|
|
|||||||||
|
Acquired Brain Injury Waiver |
|
|
|
|
|
Certification |
|
||||||||||||
|
Acquired Brain Injury/Long Term Care Waiver |
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Supports for Community Living Waiver |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Michelle P. Waiver |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Consumer Directed Option Blended |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Member admitted from (check one) |
|
|
|
|
Certification period (enter dates below) |
|
|
||||||||||||
|
Home Hospital Nursing facility |
ICF/MR/DD |
|
|
Begin date |
|
|
|
|
End date |
|
|
||||||||
|
Other: |
|
|
|
|
Certification |
number: |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Has member’s freedom of choice been explained and |
|
|
Has member been informed of the process to make |
||||||||||||||||
|
verified by a signature on the MAP 350 Form Yes |
No |
|
a complaint |
Yes |
|
No (see instructions) |
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
Physician’s name |
Physician’s license number |
Physician’s phone number |
|||||||||||||||||
|
|
|
(enter 5 digit #) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Enter member’s primary diagnosis: HCB
|
Enter all diagnoses including DSM or |
Is the member diagnosed with one of the following? |
|
|
||||||||||||||
|
AXIS I: (mental illness) |
|
Mental Retardation/ IQ= |
|
|
|
|
|
) |
|||||||||
|
|
|
|
|
|
Developmental Disability |
|
|
|
|
|
|
|
|
|
|||
|
AXIS II: (MR/DD) |
|
|
|
|
|
|
|
) |
|||||||||
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
Mental Illness |
) |
|||||||||||
|
AXIS III: (Medical) |
|
||||||||||||||||
|
|
Brain Injury |
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
Cause of Brain Injury: |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
Date of Brain Injury: |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
Rancho Scale |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION III – ASSESSMENT PROVIDER INFORMATION |
|
|
||||||||||||
|
Assessment/Reassessment provider |
Provider number |
Provider phone number |
|
|
|||||||||||||
|
name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street address |
City, state and zip code |
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Provider contact person |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page 1 of 15
MAP 351 |
Commonwealth of Kentucky |
||
(Rev. 7/08) |
Cabinet for Health and Family Services |
||
|
|
Department for Medicaid Services |
|
|
|
MEDICAID WAIVER ASSESSMENT |
|
|
|
|
|
|
NAME (LAST, FIRST) |
|
MEDICAID NUMBER |
|
|
|
|
|
|
SECTION IV SELF ASSESSMENT |
|
|
|
*For SCL, MP and ABI waivers only |
*add additional pages as needed |
Community Inclusion (what do you like to do or where would you like to go in the community, where do you go for recreation, do you not get to go somewhere that you would like to)
Relationships (How do you stay in contact with your friends and family, do you need assistance in making or keeping friends, who are your friends)
Rights (do you understand your rights, are any of your rights restricted, do you know what is abuse or neglect)
Dignity and Respect (how are you treated by staff, do you have a place you can go to be with friends or to be alone or have privacy)
Health (who are your doctors ,do you have any health concerns, what medicine do you take, how do they make you feel,)
Lifestyle (do you have a job, do you want to work, do you want to go to school, do you go to the bank, do you have spending money to carry)
Page 2 of 15
MAP 351 |
Commonwealth of Kentucky |
||||
(Rev. 7/08) |
Cabinet for Health and Family Services |
||||
|
|
|
Department for Medicaid Services |
||
|
|
|
MEDICAID WAIVER ASSESSMENT |
||
|
|
|
|
|
|
|
Name (LAST, FIRST) |
|
|
Medicaid Number |
|
|
|
|
|
|
|
|
|
|
SECTION V – ACTIVITIES OF DAILY LIVING |
||
|
1) Is member independent with |
Comments: |
|||
|
dressing/undressing |
|
|
||
|
Yes |
No(If no, check below all that apply and comment) |
|
|
|
|
Requires supervision or verbal cues |
|
|
||
|
Requires |
|
|
||
|
Requires |
|
|
||
|
Requires total assistance |
|
|
||
|
|
|
|||
|
2) Is member independent with grooming |
Comments: |
|||
|
Yes |
No(If no, check below all that apply and comment) |
|
|
|
|
Requires supervision or verbal cues |
|
|
||
|
Requires |
|
|
||
|
oral care |
shaving |
|
|
|
|
nail care |
hair |
|
|
|
|
Requires total assistance |
|
|
||
|
|
|
|||
|
3) Is member independent with bed mobility |
Comments: |
|||
|
Yes |
No (If no, check below all that apply and comment) |
|
|
|
|
Requires supervision or verbal cues |
|
|
||
|
Occasionally requires |
|
|
||
|
Always requires |
|
|
||
|
|
|
|
||
|
Required bedrails |
|
|
||
|
|
|
|||
|
4) Is member independent with bathing |
Comments: |
|||
|
Yes |
No (If no, check below all that apply and comment) |
|
|
|
|
Requires supervision or verbal cues |
|
|
||
|
Requires |
|
|
||
|
Requires |
|
|
||
|
Requires |
|
|
||
|
Requires total assistance |
|
|
||
|
|
|
|||
|
5) Is member independent with toileting |
Comments: |
|||
|
Yes |
No (If no, check below all that apply and comment) |
|
|
|
|
Bladder incontinence |
|
|
||
|
Bowel incontinence |
|
|
||
|
Occasionally requires |
|
|
||
|
Always requires |
|
|
||
|
Requires total assistance |
|
|
||
|
Bowel and bladder regimen |
|
|
||
|
|
|
|||
|
6) Is member independent with eating Yes No |
Comments: |
|||
|
(If no, check below all that apply and comment) |
|
|
||
|
Requires supervision or verbal cues |
|
|
||
|
Requires assistance cutting meat or arranging food |
|
|
||
|
Partial/occasional help |
|
|
||
|
Totally fed (by mouth) |
|
|
||
|
Tube feeding (type and tube location) |
|
|
||
|
|
|
|
|
|
Page 3 of 15
MAP 351 |
Commonwealth of Kentucky |
|||||||
(Rev. 7/08) |
Cabinet for Health and Family Services |
|||||||
|
|
|
|
Department for Medicaid Services |
||||
|
|
|
|
MEDICAID WAIVER ASSESSMENT |
||||
|
|
|
|
|
|
|
|
|
|
Name (LAST, FIRST) |
|
|
|
Medicaid Number |
|||
|
|
|
|
|
|
|
||
|
7) Is member independent with ambulation |
|
|
Comments: |
||||
|
Yes |
No (If no, check below all that apply and comment) |
|
|
|
|||
|
Dependent on device |
|
|
|
|
|
||
|
Requires aid of one person |
|
|
|
|
|
||
|
Requires aid of two people |
|
|
|
|
|
||
|
History of falls (number of falls, and date of last fall) |
|
|
|
||||
|
|
|
|
|
|
|||
|
8) Is member independent with transferring |
|
Comments: |
|||||
|
Yes |
No (If no, check below all that apply and comment) |
|
|
|
|||
|
Requires supervision or verbal cues |
|
|
|
|
|
||
|
|
|
|
|
|
|||
|
|
|
|
|
|
|||
|
Requires mechanical device |
|
|
|
|
|
||
|
Bedfast |
|
|
|
|
|
||
|
|
|
|
|
|
|||
|
|
|
SECTION VI - INSTRUMENTAL ACTIVITIES OF DAILY LIVING |
|||||
|
1) Is member able to prepare meals |
Yes |
No |
|
Comments: |
|||
|
(If no, check below all that apply and explain in the comments) |
|
|
|||||
|
Arranges for meal preparation |
|
|
|
|
|
||
|
Requires supervision or verbal cues |
|
|
|
|
|
||
|
Requires assistance with meal preparation |
|
|
|
|
|||
|
Requires total meal preparation |
|
|
|
|
|
||
|
2) Is member able to shop independently |
Yes No |
|
Comments: |
||||
|
(If no, check below all that apply and explain in the comments) |
|
|
|||||
|
Arranges for shopping to be done |
|
|
|
|
|
||
|
Requires supervision or verbal cues |
|
|
|
|
|
||
|
Requires assistance with shopping |
|
|
|
|
|
||
|
Unable to participate in shopping |
|
|
|
|
|
||
|
|
|
|
|||||
|
3) Is member able to perform light housekeeping |
|
Comments: |
|||||
|
Yes |
No |
|
|
|
|
|
|
|
(If no, check below all that apply and explain in the comments) |
|
|
|||||
|
Arranges for light housekeeping duties to be performed |
|
|
|||||
|
Requires supervision or verbal cues |
|
|
|
|
|
||
|
Requires assistance with light housekeeping |
|
|
|
|
|||
|
Unable to perform any light housekeeping |
|
|
|
|
|||
|
|
|
|
|||||
|
4) Is member able to perform heavy housework |
|
Comments: |
|||||
|
Yes |
No |
|
|
|
|
|
|
|
(If no, check below all that apply and explain in the comments) |
|
|
|||||
|
Arranges for heavy housework to be performed |
|
|
|
|
|||
|
Requires supervision or verbal cues |
|
|
|
|
|
||
|
Requires assistance with heavy housework |
|
|
|
|
|||
|
Unable to perform any heavy housework |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
Page 4 of 15
MAP 351 |
Commonwealth of Kentucky |
|
|||||||
(Rev. 7/08) |
Cabinet for Health and Family Services |
|
|||||||
|
|
|
Department for Medicaid Services |
|
|||||
|
|
|
MEDICAID WAIVER ASSESSMENT |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
Name (LAST, FIRST) |
|
|
|
Medicaid Number |
|
|||
|
|
|
|
|
|
|
|
||
|
5) Is member able to perform laundry tasks |
|
Comments: |
|
|||||
|
Yes |
No |
|
|
|
|
|
|
|
|
(If no, check below all that apply and explain in the comments) |
|
|
|
|
|
|||
|
Arranges for laundry to be done |
|
|
|
|
|
|
|
|
|
Requires supervision or verbal cues |
|
|
|
|
|
|
|
|
|
Requires assistance with laundry tasks |
|
|
|
|
|
|
|
|
|
Unable to perform any laundry tasks |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
6) Is member able to plan/arrange for |
|
Comments: |
|
|||||
|
delivery, or some means of gaining possession of |
|
|
|
|
|
|||
|
medication(s) and take them independently |
|
|
|
|
|
|||
|
Yes |
No |
|
|
|
|
|
|
|
|
(If no, check below all that apply and explain in the comments) |
|
|
|
|
|
|||
|
Arranges for medication to be obtained and taken correctly |
|
|
|
|
|
|||
|
Requires supervision or verbal cues |
|
|
|
|
|
|
|
|
|
Requires assistance with obtaining and taking medication |
|
|
|
|
|
|||
|
correctly |
|
|
|
|
|
|
|
|
|
Unable to obtain medication and take correctly |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
||
|
7) Is member able to handle finances independently |
|
Comments: |
|
|||||
|
Yes |
No |
|
|
|
|
|
|
|
|
(If no, check below all that apply and explain in the comments) |
|
|
|
|
|
|||
|
Arranges for someone else to handle finances |
|
|
|
|
|
|||
|
Requires supervision or verbal cues |
|
|
|
|
|
|
|
|
|
Requires assistance with handling finances |
|
|
|
|
|
|||
|
Unable to handle finances |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
8) Is member able to use the telephone independently |
|
Comments: |
|
|||||
|
Yes |
No |
|
|
|
|
|
|
|
|
(If no, check below all that apply and explain in the comments) |
|
|
|
|
|
|||
|
Requires adaptive device to use telephone |
|
|
|
|
|
|||
|
Requires supervision or verbal cues |
|
|
|
|
|
|
|
|
|
Requires assistance when using telephone |
|
|
|
|
|
|||
|
Unable to use telephone |
|
|
|
|
|
|
|
|
|
|
SECTION |
|
||||||
|
1) Does member exhibit behavior problems |
|
Comments: |
|
|
||||
|
Yes |
No (If yes, check below all that apply and explain |
|
Date of functional analysis: |
and/or |
||||
|
the frequency in comments) |
|
|
Date of behavior support plan: |
|
||||
|
|
|
|
|
|
|
|
||
|
Disruptive behavior |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Agitated behavior |
|
|
|
|
|
|
|
|
|
Assaultive behavior |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
Page 5 of 15
MAP 351 |
Commonwealth of Kentucky |
|
(Rev. 7/08) |
Cabinet for Health and Family Services |
|
|
Department for Medicaid Services |
|
|
MEDICAID WAIVER ASSESSMENT |
|
|
|
|
Name (LAST, FIRST) |
|
Medicaid Number |
|
|
|
2) Is member oriented to person, place, time |
Comments: |
|
Yes No (If no, check below all that apply and comment) |
|
|
Forgetful |
|
|
Confused |
|
|
Unresponsive |
|
|
Impaired Judgment |
|
|
|
|
|
3) Has member experienced a major change or |
Description: |
|
crisis within the past twelve months |
Yes No |
|
(If yes, describe) |
|
|
|
|
|
4) Is the member actively participating in social |
Description: |
|
and/or community activities Yes |
No |
|
(If yes, describe) |
|
|
|
|
|
5) Is the member experiencing any of the following |
Comments: |
|
(For each checked, explain the frequency and details in the |
|
|
comments section) |
|
|
Difficulty recognizing others |
|
|
Loneliness |
|
|
Sleeping problems |
|
|
Anxiousness |
|
|
Irritability |
|
|
Lack of interest |
|
|
|
|
|
|
|
|
Hopelessness |
|
|
Suicidal behavior |
|
|
Medication abuse |
|
|
Substance abuse |
|
|
Alcohol Abuse |
|
|
Page 6 of 15

MAP 351 |
Commonwealth of Kentucky |
|
(Rev. 7/08) |
Cabinet for Health and Family Services |
|
|
Department for Medicaid Services |
|
|
MEDICAID WAIVER ASSESSMENT |
|
|
|
|
Name (LAST, FIRST) |
Medicaid Number |
|
|
|
|
6) Cognitive functioning (Participant’s current |
Comments: |
|
level of alertness, orientation, comprehension, |
|
|
concentration, and immediate memory for simple |
|
|
commands) |
|
|
|
Alert/oriented, able to focus and shift |
|
attention, comprehends and recalls task |
|
|
directions independently. |
|
|
|
Requires prompting (cueing, repetition, |
|
reminders) only under stressful or unfamiliar |
|
|
conditions. |
|
|
|
Requires assistance and some direction in |
|
|
specific situations (e.g., on all tasks |
|
|
involving shifting of attention), or |
|
|
consistently requires low stimulus |
|
|
environment due to distractibility. |
|
|
Required considerable assistance in routine |
|
|
situations. Is not alert and oriented or is |
|
|
unable to shift attention and recall directions |
|
|
more than half the time. |
|
|
Totally dependent due to disturbances such |
|
|
as constant disorientation, coma, persistent |
|
|
vegetative state, or delirium. |
|
|
|
|
7) When Confused (Reported or Observed): |
Comments: |
|
|
Never |
|
|
In new or complex situations only |
|
|
On awakening or at night only |
|
|
During the day and evening, but not |
|
constantly |
|
|
|
Constantly |
|
|
NA |
|
|
|
|
8) When Anxious (Reported or Observed): |
Comments: |
|
|
None of the time |
|
|
Less often than daily |
|
|
Daily, but not constantly |
|
|
All of the time |
|
|
NA |
|
|
|
|
9) Depressive Feelings (Reported or Observed): |
Comments: |
|
|
Depressed mood (e.g., feeling sad, tearful) |
|
|
Sense of failure or |
|
|
Hopelessness |
|
|
Recurrent thoughts of death |
|
|
Thoughts of suicide |
|
|
None of the above feelings reported or |
|
observed |
|
|
|
|
|
Page 7 of 15

MAP 351 |
Commonwealth of Kentucky |
|
(Rev. 7/08) |
Cabinet for Health and Family Services |
|
|
Department for Medicaid Services |
|
|
MEDICAID WAIVER ASSESSMENT |
|
|
|
|
Name (LAST, FIRST) |
Medicaid Number |
|
|
|
|
10) Member Behaviors (Reported or Observed): |
Comments: |
|
|
Indecisiveness, lack of concentration |
|
|
Diminished interest in most activities |
|
|
Sleep disturbances |
|
|
Recent changes in appetite or weight |
|
|
Agitation |
|
|
Suicide attempt |
|
|
None of the above behaviors observed or |
|
reported |
|
|
|
|
|
11) Behaviors Demonstrated at Least Once a |
Comments: |
|
Week: |
Memory deficit: failure to recognize |
|
|
|
|
|
familiar persons/places, inability to recall |
|
|
events of past |
|
|
loss so that supervision is required. |
|
|
Impaired |
|
|
perform usual ADL’s, inability to |
|
|
inappropriately stop activities, jeopardizes |
|
|
safety through actions. |
|
|
Verbal disruption: yelling, threatening, |
|
|
excessive profanity, sexual references, etc. |
|
|
Physical aggression: aggressive or |
|
|
combative to self and others (e.g. hits self, |
|
|
throws objects, punches, dangerous |
|
|
maneuvers with wheelchair or other |
|
|
objects). |
|
|
Disruptive, infantile, or socially |
|
|
inappropriate behavior (excludes verbal |
|
|
actions). |
|
|
Delusional, hallucinatory, or paranoid |
|
|
behavior. |
|
|
None of the above behaviors demonstrated. |
|
|
|
|
12 ) Frequency of Behavior Problems (Reported or |
Comments: |
|
Observed) such as wandering episodes, self abuse, |
|
|
verbal disruption, physical aggression, etc.: |
|
|
|
Never |
|
|
Less than once a month |
|
|
Once a month |
|
|
Several times each month |
|
|
Several times a week |
|
|
At least daily |
|
|
|
|
Page 8 of 15

MAP 351 |
|
Commonwealth of Kentucky |
|||
(Rev. 7/08) |
|
Cabinet for Health and Family Services |
|||
|
|
|
|
Department for Medicaid Services |
|
|
|
|
|
MEDICAID WAIVER ASSESSMENT |
|
|
|
|
|
||
|
Name (LAST, FIRST) |
|
Medicaid Number |
||
|
|
|
|
|
|
13) |
Mental Status: |
|
Comments: |
||
|
|
|
Oriented |
|
|
|
|
|
Forgetful |
|
|
|
|
|
Depressed |
|
|
|
|
|
Disoriented |
|
|
|
|
|
Lethargic |
|
|
|
|
|
Agitated |
|
|
|
|
|
Other |
|
|
|
|
|
|||
|
14) Is this member receiving Psychiatric Nursing |
Comments: |
|||
|
Services at home provided by a qualified psychiatric |
|
|||
|
nurse? |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
SECTION |
|
|
1) Is member’s vision adequate (with or without |
Comments: |
|||
|
glasses) |
|
|
|
|
|
Yes |
No |
Undetermined |
|
|
|
(If no, check below all that apply and comment) |
|
|||
|
Difficulty seeing print |
|
|||
|
Difficulty seeing objects |
|
|||
|
No useful vision |
|
|
||
|
|
|
|||
|
2) Is member’s hearing adequate (with or without |
Comments: |
|||
|
hearing aid) |
|
|
|
|
|
Yes |
No |
Undetermined |
|
|
|
(If no, check below all that apply, and comment) |
|
|||
|
Difficulty with conversation level |
|
|||
|
Only hears loud sounds |
|
|||
|
No useful hearing |
|
|
||
|
|
|
|||
|
3) Is member able to communicate needs |
Comments: |
|||
|
Yes |
No (If no, check below all that apply and comment) |
|
||
|
Speaks with difficulty but can be understood |
|
|||
|
Uses sign language and/or gestures/communication device |
|
|||
|
Inappropriate context |
|
|
||
|
Unable to communicate |
|
|||
|
|
|
|||
|
4) Does member maintain an adequate diet |
Comments: |
|||
|
Yes |
No (If no, check all that apply and comment) |
|
||
|
Uses dietary supplements |
|
|||
|
Requires special diet (low salt, low fat, etc.) |
|
|||
|
Refuses to eat |
|
|
||
|
Forgets to eat |
|
|
||
|
Tube feeding required (Explain the brand, amount, and |
|
|||
|
frequency in the comments section) |
|
|||
|
Other dietary considerations (PICA, |
|
|||
|
|
|
|
|
|
Page 9 of 15
| Fact Name | Description |
|---|---|
| Form Title | Kentucky Map 351 - Medicaid Waiver Assessment |
| Governing Body | Cabinet for Health and Family Services, Department for Medicaid Services |
| Revision Date | Revised in July 2008 |
| Member Demographics | Includes name, date of birth, Medicaid ID, address, and emergency contact information. |
| Waiver Eligibility | Determines eligibility for various Medicaid waiver programs such as Home and Community Based Waiver. |
| Assessment Provider Information | Captures details about the assessment provider, including name and contact information. |
| Activities of Daily Living | Assesses the member's independence in daily activities like dressing, grooming, and eating. |
| Instrumental Activities of Daily Living | Evaluates the member's ability to perform tasks such as meal preparation and managing finances. |
| Behavioral Assessment | Identifies any behavioral issues and includes a functional analysis date and behavior support plan date. |
Once you have the Kentucky Map 351 form in front of you, it’s time to fill it out accurately. This process requires attention to detail to ensure that all necessary information is provided. Here are the steps to complete the form:
What is the Kentucky Map 351 form?
The Kentucky Map 351 form is a Medicaid Waiver Assessment used to determine eligibility for various Medicaid waiver programs in Kentucky. It collects important information about the member, including demographics, health status, and daily living activities. The form is essential for assessing the needs of individuals who require assistance due to disabilities or other health conditions.
Who needs to fill out the Map 351 form?
The form must be completed for individuals applying for or renewing their eligibility for Medicaid waiver programs. This includes those seeking support through Home and Community Based Waivers, Acquired Brain Injury Waivers, and others. It is typically filled out by the member or their representative, with input from healthcare providers as needed.
What information is required on the Map 351 form?
The form requires a variety of information, including:
How does the assessment process work?
The assessment process involves evaluating the member’s needs and capabilities. After completing the Map 351 form, a qualified provider will review the information and may conduct an in-person assessment. This assessment helps to determine the level of care and support the member requires. The results will influence the approval of the waiver application.
What happens after submitting the Map 351 form?
Once the Map 351 form is submitted, the relevant Medicaid authority will review the application. If additional information is needed, they may contact the member or their representative. After the review, a determination will be made regarding eligibility for the requested waiver program. Members will be notified of the decision, and if approved, they will receive further instructions on accessing services.
Filling out the Kentucky Map 351 form can be a daunting task, and mistakes are common. One of the most frequent errors occurs when individuals fail to provide complete and accurate demographic information. Missing details such as the member’s full name, date of birth, or Medicaid Member ID can lead to significant delays in processing. Ensuring that all fields are filled out correctly is essential to avoid unnecessary complications.
Another common mistake is neglecting to check the appropriate boxes for the member’s marital status and sex. This seemingly minor oversight can create confusion during the eligibility assessment. It’s important to double-check these sections to ensure that the information aligns with the member’s current status.
Many people also overlook the importance of providing a primary diagnosis and additional diagnoses with the correct codes. This information is crucial for determining eligibility for specific waivers. Without accurate diagnosis codes, the assessment may not reflect the member’s true needs, which can impact their access to necessary services.
In Section II, a common error is failing to indicate whether the member's freedom of choice has been explained and verified. This is a critical requirement, and neglecting to sign off on this can result in the application being rejected. It’s essential to ensure that all necessary signatures are obtained and documented properly.
When it comes to the assessment of daily living activities, individuals often misinterpret the instructions. For example, when answering whether the member is independent with activities like dressing or bathing, it’s vital to provide honest and detailed comments. Misrepresenting the level of assistance needed can lead to inappropriate service allocation.
Another frequent mistake is not providing enough detail in the self-assessment section. This area allows members to express their preferences and needs, and vague responses can hinder the assessment process. Specific examples of community involvement or relationships can help assessors understand the member’s situation better.
In the instrumental activities of daily living section, many people fail to indicate whether the member can handle finances or use the telephone independently. These skills are essential for assessing overall independence. Providing clear comments about the member’s capabilities can significantly influence their eligibility and the services they receive.
Additionally, some applicants do not keep track of important dates, such as the date of brain injury or the last functional analysis. This information is crucial for evaluating the member’s needs and ensuring that the assessment is up-to-date. Keeping thorough records can prevent complications later in the process.
Lastly, individuals sometimes submit the form without reviewing it for completeness. A final check can catch errors that might have been overlooked during the initial filling out of the form. Taking a moment to ensure that all sections are complete and accurate can save time and frustration in the long run.
By being aware of these common mistakes, applicants can improve their chances of a smooth and successful application process. Attention to detail and thoroughness are key when completing the Kentucky Map 351 form.
The Kentucky Map 351 form serves as a vital component in the Medicaid waiver assessment process. However, it is often accompanied by several other forms and documents that help create a comprehensive profile for individuals seeking assistance. Each of these documents plays a unique role in ensuring that the assessment process is thorough and effective.
In summary, the Kentucky Map 351 form, while significant, is part of a larger framework of documentation that ensures individuals receive the appropriate support and care they need. Each accompanying document contributes to a holistic understanding of the member's situation, facilitating a smoother and more effective assessment process.
When filling out the Kentucky Map 351 form, it’s important to follow specific guidelines to ensure accuracy and completeness. Here’s a list of things you should and shouldn’t do:
Here are nine common misconceptions about the Kentucky Map 351 form, along with clarifications to help you understand its purpose and requirements.
This form is also used for re-certifications and re-applications, making it essential for ongoing Medicaid eligibility.
In fact, the form requires comprehensive medical history, including diagnoses and treatment details, to assess eligibility accurately.
Only authorized individuals, such as healthcare providers or case managers, should complete the form to ensure accuracy and compliance.
Additional documentation may be needed, including the MAP 350 form, which verifies the member’s freedom of choice and complaint process.
While it may seem simple, the form has multiple sections that require careful attention to detail. Incomplete or incorrect information can delay processing.
A physician's signature is essential to validate the medical information provided and confirm the member’s diagnosis.
This form is applicable to a range of individuals who may require various levels of support, not just those with severe disabilities.
Processing times can vary significantly based on the completeness of the application and the current workload of the Medicaid office.
There is a process for appeals, and understanding your rights and options is crucial if you receive a denial.
Filling out the Kentucky Map 351 form is an important step in the Medicaid waiver assessment process. Here are key takeaways to consider:
By following these guidelines, you can help ensure that the Kentucky Map 351 form is completed correctly, facilitating a smoother assessment process for Medicaid waivers.