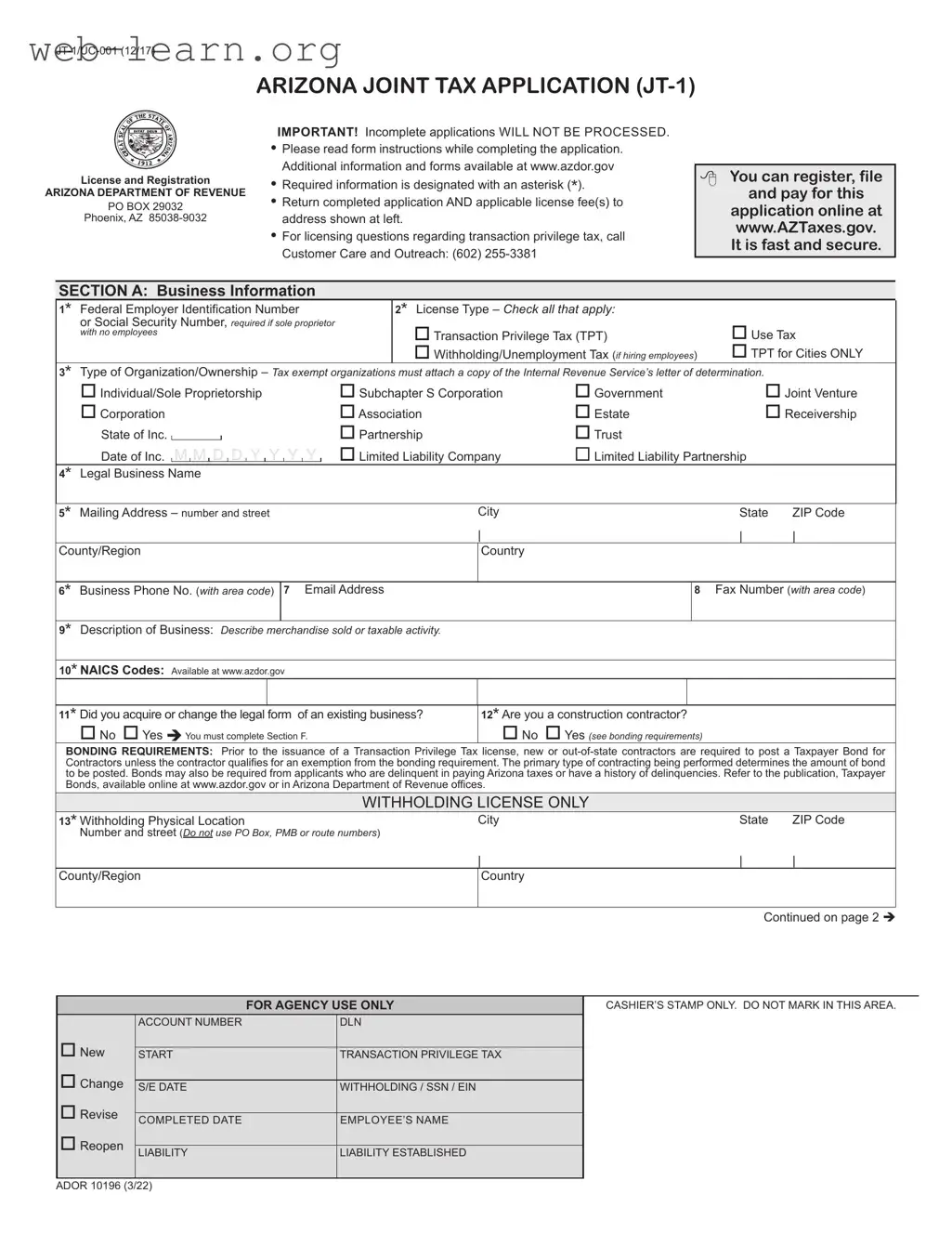
The Arizona Joint Tax Application, commonly referred to as the JT-1 form, plays a crucial role for businesses operating within the state. This form is essential for those seeking to apply for various tax licenses, including Transaction Privilege Tax (TPT), Use Tax, and Employer Withholding and Unemployment Insurance. Designed to streamline the licensing process, the JT-1 form allows business owners to register their enterprises, report changes in ownership, and update their legal business structure. It includes several sections that require detailed information about the business, such as its legal name, ownership structure, and contact details. Additionally, applicants must provide their Federal Employer Identification Number (FEIN) or Social Security Number, along with a description of their business activities. The form also addresses specific requirements for construction contractors, including bonding obligations, and outlines the necessary fees associated with licensing. To ensure a smooth application process, it is vital to complete the form accurately and attach any required documentation. By understanding the key aspects of the JT-1 form, business owners can navigate the tax licensing landscape in Arizona more effectively.
ARIZONA JOINT TAX APPLICATION
License and Registration
ARIZONA DEPARTMENT OF REVENUE
PO BOX 29032
Phoenix, AZ
IMPORTANT! Incomplete applications WILL NOT BE PROCESSED.
•Please read form instructions while completing the application. Additional information and forms available at www.azdor.gov
•Required information is designated with an asterisk (*).
•Return completed application AND applicable license fee(s) to address shown at left.
•For licensing questions regarding transaction privilege tax, call Customer Care and Outreach: (602)
You can register, file
and pay for this
application online at www.AZTaxes.gov. It is fast and secure.
SECTION A: Business Information
1* Federal Employer Identification Number
or Social Security Number, required if sole proprietor with no employees
2* License Type – Check all that apply: |
|
Transaction Privilege Tax (TPT) |
Use Tax |
Withholding/Unemployment Tax (if hiring employees) |
TPT for Cities ONLY |
3* Type of Organization/Ownership – Tax exempt organizations must attach a copy of the Internal Revenue Service’s letter of determination.
Individual/Sole Proprietorship |
Subchapter S Corporation |
Government |
Joint Venture |
||
Corporation |
Association |
Estate |
Receivership |
||
State of Inc. |
|
|
Partnership |
Trust |
|
Date of Inc. M M D D Y Y Y Y |
Limited Liability Company |
Limited Liability Partnership |
|
||
|
|
|
|
|
|
4* Legal Business Name
5* Mailing Address – number and street |
City |
State |
ZIP Code |
||||
|
|
|
| |
|
|
| |
| |
County/Region |
Country |
|
|
||||
|
|
|
|
|
|
|
|
6* Business Phone No. (with area code) |
7 Email Address |
|
|
8 |
Fax Number (with area code) |
||
|
|
|
|
|
|
|
|
9* Description of Business: Describe merchandise sold or taxable activity. |
|
|
|
|
|
||
|
|
|
|
|
|
||
10* NAICS Codes: Available at www.azdor.gov |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
11* Did you acquire or change the legal form of an existing business? |
12* Are you a construction contractor? |
|
|
||||
No Yes You must complete Section F. |
No Yes (see bonding requirements) |
|
|
||||
BONDING REQUIREMENTS: Prior to the issuance of a Transaction Privilege Tax license, new or
WITHHOLDING LICENSE ONLY
13* Withholding Physical Location |
City |
State |
ZIP Code |
Number and street (Do not use PO Box, PMB or route numbers) |
|
|
|
|
| |
| |
| |
County/Region |
Country |
|
|
|
|
|
|
Continued on page 2
FOR AGENCY USE ONLY
CASHIER’S STAMP ONLY. DO NOT MARK IN THIS AREA.
New
Change
Revise
Reopen
ACCOUNT NUMBER |
DLN |
|
|
START |
TRANSACTION PRIVILEGE TAX |
|
|
S/E DATE |
WITHHOLDING / SSN / EIN |
|
|
COMPLETED DATE |
EMPLOYEE’S NAME |
|
|
LIABILITY |
LIABILITY ESTABLISHED |
|
|
ADOR 10196 (3/22)
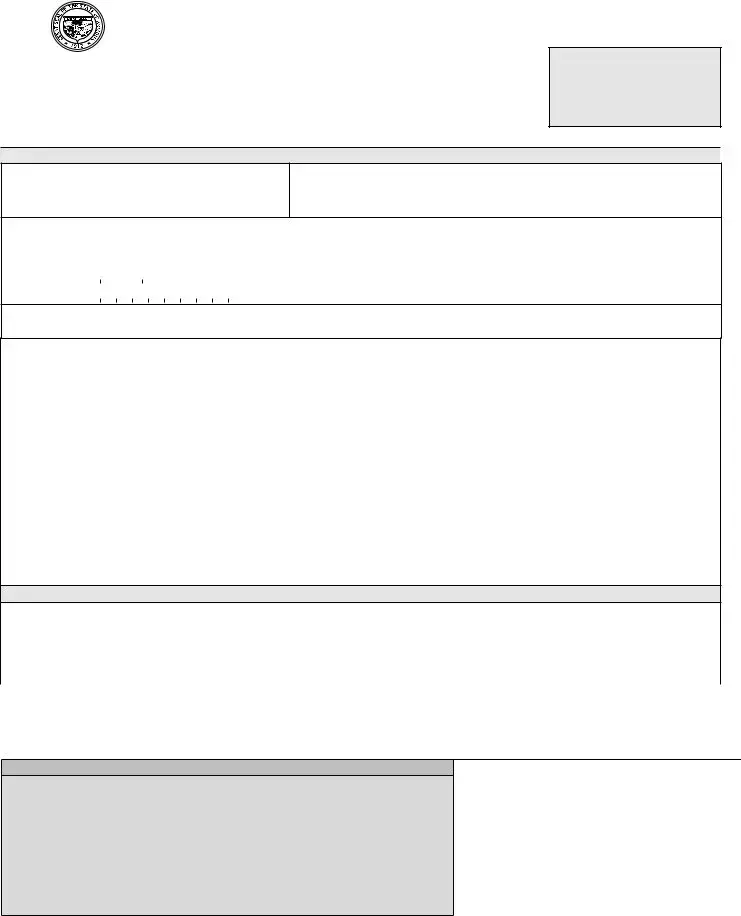
Name (as shown on page 1)
FEIN or SSN (as shown on page 1)
SECTION B: Identification of Owners, Partners, Corporate Officers Members/Managing Members or Officials of this Employing Unit
If you need more space, attach Additional Owner, Partner, Corporate Officer(s) form available at www.azdor.gov. If the owner, partners, corporate officers or combination of partners or corporate officers, members and/or managing members own more than 50% of or control another business in Arizona, attach a list of the businesses, percentages owned and unemployment insurance account numbers or provide a Power of Attorney (Form 285) which must be filled out and signed by an authorized corporate officer.
|
*Social Security No. |
|
*Title |
1 |
|
|
|
Owner |
*Street Address |
|
|
*ZIP Code |
|
*County |
|
|
|||
|
|
||
|
*Social Security No. |
|
*Title |
|
|
||
|
|
||
2 |
|
|
|
Owner |
*Street Address |
|
|
*ZIP Code |
|
*County |
|
|
|||
|
|
||
|
*Social Security No. |
|
*Title |
|
|
||
|
|
||
3 |
|
|
|
Owner |
*Street Address |
|
|
*ZIP Code |
|
*County |
|
|
|||
|
|
||
|
|
|
|
*Last Name |
First Name |
Middle Intl. |
||
| |
|
|
|
| |
*City |
|
|
*State |
* % Owned |
|
|
|
|
|
*Phone Number (with area code) |
|
*Country |
|
|
|
|
|
|
|
*Last Name |
First Name |
Middle Intl. |
||
| |
|
|
|
| |
*City |
|
|
*State |
* % Owned |
|
|
|
|
|
*Phone Number (with area code) |
|
*Country |
|
|
|
|
|
|
|
*Last Name |
First Name |
Middle Intl. |
||
| |
|
|
|
| |
*City |
|
|
*State |
* % Owned |
|
|
|
|
|
*Phone Number (with area code) |
|
*Country |
|
|
|
|
|
|
|
SECTION C: Transaction Privilege Tax (TPT)
1* Date Business Started in Arizona 2* Date Sales Began |
3 What is your Estimated Tax Liability for your first twelve months of business? |
|
M |
|
M |
|
D |
|
D |
|
Y |
|
Y |
|
Y |
|
Y |
M |
|
M |
|
D |
|
D |
|
Y |
|
Y |
|
Y |
|
Y |
|
|
|
||
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
4 |
Filing Frequency Monthly |
Quarterly |
|
Seasonal Annual |
If seasonal filer, check the months for which you intend to do business: |
||||||||||||||||||||||||||||||
|
JAN FEB MAR |
APR MAY |
JUN JUL |
AUG |
SEP OCT NOV DEC |
||||||||||||||||||||||||||||||
5 |
Does your business sell tobacco products? |
|
6 |
TPT Filing Method |
|
7 |
Does your business sell new motor vehicle tires or vehicles? |
||||||||||||||||||||||||||||
|
Yes Retailer OR Distributor |
|
|
|
|
|
|
|
Cash Receipts |
|
|
Yes You will have to file Motor Vehicle Tire Fee form |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accrual |
|
|
available at www.azdor.gov |
||||||
8* Tax Records Physical Location – number and street |
|
|
|
|
|
|
City |
State ZIP Code |
|||||||||||||||||||||||||||
|
(Do not use PO Box, PMB or route numbers) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
County
9* Name of Contact
| |
| |
Country |
|
* Phone Number (with area code) |
Extension |
|
| |
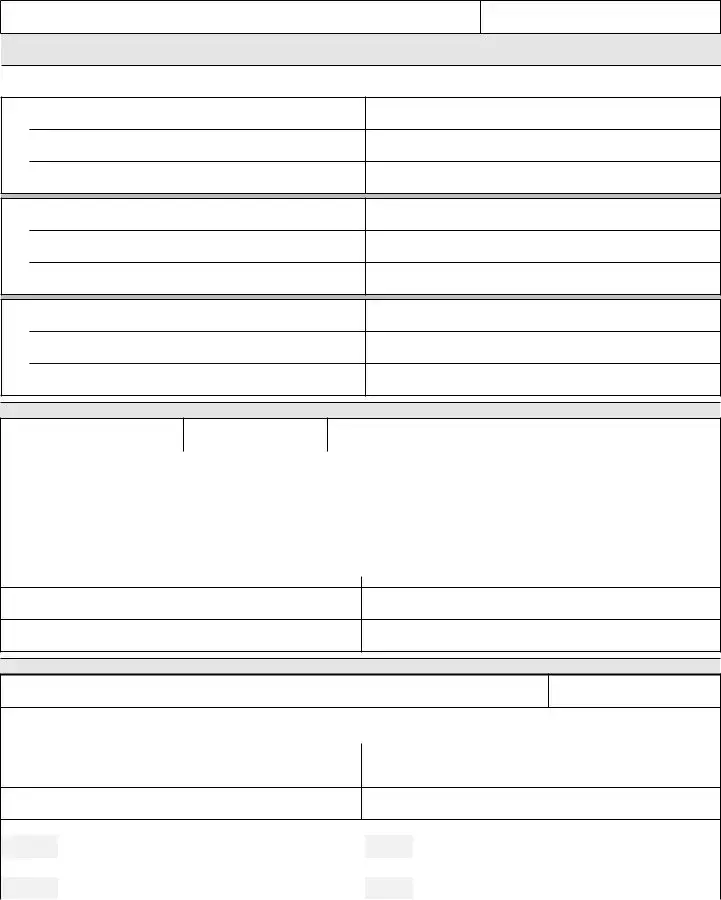
SECTION D: Transaction Privilege Tax (TPT) Physical Location
1* Business Name, “Doing Business As” or Trade Name at this Physical Location
2* Phone Number (with area code)
3* Physical Location of Business or Commercial/Residential Rental |
City |
State |
ZIP Code |
Number and street (Do not use PO Box, PMB or route numbers) |
|
|
|
|
|
| |
| |
County/Region |
Country |
|
|
Residential Rental Only – Number of Units
Reporting City (if different than the physical location city)
4* Additional County/Region Indian Reservation/City: County/Region Indian Reservation and City Codes available at www.azdor.gov
County/ |
|
|
|
|
|
|
|
|
|
|
Region |
|
|
|
|
|
City |
|
|
|
|
Business Codes (Include all codes that apply): |
See instructions. Complete list available at www.azdor.gov |
|||||||||
State/ |
|
|
|
|
|
|
|
|
|
|
County |
|
|
|
|
|
City |
|
|
|
|
If you have more locations, attach Additional Business Locations form available at www.azdor.gov
ADOR 10196 (3/22) |
ARIZONA JOINT TAX APPLICATION |
Page 2 of 4 |
Name (as shown on page 1)
FEIN or SSN (as shown on page 1)
SECTION E: Withholding & Unemployment Tax Applicants
1* Regarding THIS application, Date Employees First Hired in Arizona |
2 |
Are you liable for Federal Unemployment Tax? |
||||||||||||
|
M M |
|
D D |
|
Y Y Y Y |
|
Yes First year of liability: Y |
|
Y |
|
Y |
|
Y |
|
|
|
|
||||||||||||
3 Are individuals performing services that are excluded from withholding |
4 |
Do you have an IRS ruling that grants an exclusion from |
||||||||||||
or unemployment tax? |
|
Federal Unemployment Tax? |
||||||||||||
Yes Describe services: |
|
Yes Attach a copy of the Ruling Letter. |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5Do you have, or have you previously had, an Arizona unemployment tax number?
|
No |
|
|
|
Unemployment Tax Number: |
||||
|
Yes Business Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
First calendar quarter Arizona employees were/will be hired and paid |
Hired Year |
Hired Quarter |
|
|
Paid Year |
Paid Quarter |
||
|
(indicate quarter as 1, 2, 3, 4): |
Y Y Y Y |
Q |
|
Y Y Y Y |
Q |
|||
|
|
|
|
||||||
7 |
When did/will you first pay a total of $1,500 or more gross wages in a calendar quarter? |
|
|
|
Year |
Quarter |
|||
|
(indicate quarter as 1, 2, 3, 4) |
|
|
|
|
|
|
|
|
|
|
|
|
Y Y Y Y |
Q |
||||
|
Exceptions: $20,000 gross cash wages Agricultural; $1,000 gross cash wages Domestic/Household; not applicable to 501(c)(3) |
|
|||||||
8 |
When did/will you first reach the 20th week of employing 1 or more individuals for some portion of a day in |
|
|
Year |
Quarter |
||||
|
each of 20 different weeks in the same calendar year? (indicate quarter as 1, 2, 3, 4) |
|
|
Y Y Y Y |
Q |
||||
|
Exceptions: 10 or more individuals Agricultural; 4 or more individuals 501(c)(3) |
|
|||||||
|
|
|
|
|
|
|
|
|
|
SECTION F: Acquired Business Information
If you answered “Yes” to Section A, question 11, you must complete Section F.
1* Did you acquire or change all or part of an existing business? |
2* |
|
Date of Acquisition |
3* EIN of Business Under Previous Owner |
||||||||||||||||||||||||||||
All |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Part |
|
|
M |
|
M |
|
D |
|
D |
|
|
Y |
|
|
Y |
|
|
Y |
|
|
Y |
|
||||||||||
|
|
|
|
|
|
|||||||||||||||||||||||||||
4* Previous Owner’s Telephone Number |
5* Name of Business Under Previous Owner |
6* Name of Previous Owner |
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7* Did you change the legal form of all or part of the Arizona operations of |
|
8* |
|
|
|
Date of Change |
9* EIN of Previous Legal Form |
|||||||||||||||||||||||||
your existing business? (e.g., change from sole proprietor to corporation or etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
All |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Part |
|
|
M |
|
M |
|
D |
|
D |
|
Y |
|
Y |
|
Y |
|
Y |
|
||||||||||||||
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION G: AZTaxes.gov Security Administrator
Visit www.AZTaxes.gov (the Arizona Department of Revenue’s online customer service center) to register for online services. The authorized individual will have full online access to transaction privilege, use, withholding and corporate tax account information and services. The authorized individual will be able to add or delete users and grant user privileges. Online services include viewing tax account information, filing tax returns, signing returns electronically with a
SECTION H: Required Signatures
This application must be signed by either a sole owner, at least two partners, managing member or corporate officer legally responsible for the business, trustee or receiver or representative of an estate that has been listed in Section B.
1 Print or Type Name
2 Print or Type Name
Title
Title
Date
Date
Signature
Signature
This application must be completed, signed, and returned as provided by A.R.S. §
Equal Opportunity Employer/Program
This application is available in alternative formats at Unemployment Insurance Tax Office.
PLEASE COMPLETE SECTION I: STATE/COUNTY & CITY LICENSE FEE WORKSHEET
TO CALCULATE AND REMIT TOTAL AMOUNT DUE WITH THIS APPLICATION.
ADOR 10196 (3/22) |
ARIZONA JOINT TAX APPLICATION |
Page 3 of 4 |
| Fact Name | Details |
|---|---|
| Form Purpose | The JT-1 Arizona Tax Form is used to apply for Transaction Privilege Tax, Use Tax, and Employer Withholding and Unemployment Insurance. |
| Governing Law | This form is governed by Arizona Revised Statutes § 23-722, which outlines the requirements for tax applications. |
| Required Information | Applicants must provide specific information marked with an asterisk (*), including their Federal Employer Identification Number or Social Security Number. |
| Application Submission | Incomplete applications will not be processed. It's crucial to return the completed application along with any applicable license fees to the address provided. |
| Online Services | Individuals can register, file, and pay for this application online at www.AZTaxes.gov, making the process fast and secure. |
Filling out the Jt 1 Arizona Tax form requires attention to detail. It is important to ensure that all required sections are completed accurately to avoid processing delays. After submitting the form, you can expect to receive further communication from the Arizona Department of Revenue regarding your application status.
The JT-1 Arizona Tax form is used to apply for various tax licenses in Arizona, including the Transaction Privilege Tax (TPT), Use Tax, and Employer Withholding and Unemployment Insurance. This form is essential for businesses that sell products or provide services subject to these taxes.
Any individual or organization planning to operate a business in Arizona that involves sales or services subject to taxation must complete the JT-1 form. This includes sole proprietors, corporations, partnerships, and other business entities.
Key information required includes:
All required fields are marked with an asterisk (*) and must be filled out to avoid processing delays.
Yes, businesses can register, file, and pay for the application online at www.AZTaxes.gov. This online process is designed to be fast and secure.
New or out-of-state contractors must post a Taxpayer Bond for Contractors before obtaining a Transaction Privilege Tax license. The bond amount depends on the type of contracting performed. Exemptions may apply, and further details can be found in the publication, Taxpayer Bonds, available online.
To check the status of your application, you may contact the Arizona Department of Revenue's Customer Care and Outreach at (602) 255-3381. They can provide updates and assist with any questions regarding your application.
If you need to update your business information, you should complete a Business Account Update form. This form can be found on the Arizona Department of Revenue's website. Ensure to include the applicable fees related to the updates.
Yes, there are fees associated with the JT-1 form. The total amount due includes state and city license fees, which vary based on the number of business locations and the specific city or county regulations. A worksheet is provided within the form to help calculate the total fees.
Submitting an incomplete application will result in delays. The Arizona Department of Revenue will not process applications that lack required information. It is crucial to review the form and instructions carefully before submission.
Additional information and resources can be found on the Arizona Department of Revenue's website at www.azdor.gov. For specific questions, you may also reach out to their Customer Service Center during business hours.
Filling out the JT-1 Arizona Tax form can be a daunting task, and many applicants inadvertently make mistakes that can delay the processing of their applications. One common mistake is failing to provide complete information. Every section marked with an asterisk (*) is required, and leaving any of these fields blank can lead to an automatic rejection of the application. It’s crucial to double-check that all required information is filled out accurately before submission.
Another frequent error is neglecting to read the form instructions thoroughly. The instructions are designed to guide applicants through the process and ensure that all necessary details are included. Ignoring these instructions can result in missing vital information or misinterpreting what is required. Taking the time to read through the guidelines can save significant time and frustration later on.
Many applicants also overlook the importance of providing a valid mailing address. The JT-1 form requires a complete mailing address, including the city, state, and ZIP code. Failing to provide this information correctly can lead to miscommunication or delays in receiving important documents related to the application. Ensure that the address is current and accurate to avoid any complications.
Additionally, some individuals mistakenly assume that they can submit the application without including the appropriate license fees. The form explicitly states that the completed application must be returned along with the applicable fees. Not including the correct payment can result in the application being processed only after the fees are received, which can extend the timeline significantly.
Lastly, many applicants forget to sign the application. The JT-1 form must be signed by an authorized individual, such as a sole owner, partner, or corporate officer. An unsigned application will not be considered valid and will not be processed. Taking the time to ensure that all signatures are in place is a simple yet essential step in the application process.
The Arizona Joint Tax Application (JT-1) is a crucial document for businesses in Arizona seeking to apply for various tax licenses. When completing this form, several other documents may also be necessary to ensure compliance with state regulations. Below is a list of commonly used forms that accompany the JT-1.
Having these documents ready can help streamline the application process for the JT-1 form. Ensure all information is accurate and complete to avoid any delays in processing.
Filling out the JT-1 Arizona Tax form can seem daunting, but following some straightforward guidelines can help ensure your application is processed smoothly. Here’s a list of things you should and shouldn't do:
By keeping these tips in mind, you can navigate the application process with confidence and clarity. Remember, attention to detail is key!
This is not true. The JT-1 form is designed for all types of businesses, regardless of size. Whether you are a sole proprietor or a large corporation, if you engage in activities that require a transaction privilege tax, you must complete this application.
In fact, incomplete applications will not be processed. Every section marked with an asterisk (*) is required, and omitting any of this information can lead to delays or rejection of your application.
While mailing the form is an option, businesses can also register, file, and pay for the application online at www.AZTaxes.gov. This method is often faster and more secure.
This is incorrect. The form is applicable to any business engaging in taxable activities, including services. If your business provides a service subject to tax, you are required to complete the JT-1.
Even sole proprietors must provide a Federal Employer Identification Number (FEIN) or Social Security Number (SSN) when completing the JT-1 form. This information is crucial for tax processing and identification purposes.
In reality, there are applicable license fees associated with the application. It is important to complete the State/County & City License Fee Worksheet included in the form to calculate the total amount due.
When filling out the Jt 1 Arizona Tax form, it’s crucial to pay attention to detail. Here are some key takeaways to keep in mind:
By following these guidelines, you can streamline the process of filling out and submitting the Jt 1 Arizona Tax form. Good luck!