The Illinois HFS 2243 form serves as a crucial component in the provider enrollment process for the Illinois Medical Assistance Program. This application is designed for healthcare providers seeking to enroll, re-enroll, or update their information within the program. It is essential that all sections of the form are completed accurately; incomplete applications may be returned, delaying the enrollment process. The form requires basic information such as the provider's name, type, and primary office address, as well as specific identifiers like the National Provider Identification number and any relevant licenses or certifications. Additionally, providers must detail their service categories and specialties, including any hospital admitting privileges if applicable. The form also includes sections for former participation and payee information, ensuring that all necessary financial details are captured. Finally, a certification section emphasizes the importance of providing truthful information, with an acknowledgment of potential legal consequences for any discrepancies. Overall, the Illinois HFS 2243 form is a comprehensive document that facilitates the enrollment of healthcare providers into a vital state program, ensuring that they meet all regulatory requirements.
State of Illinois
Department of Healthcare and Family Services
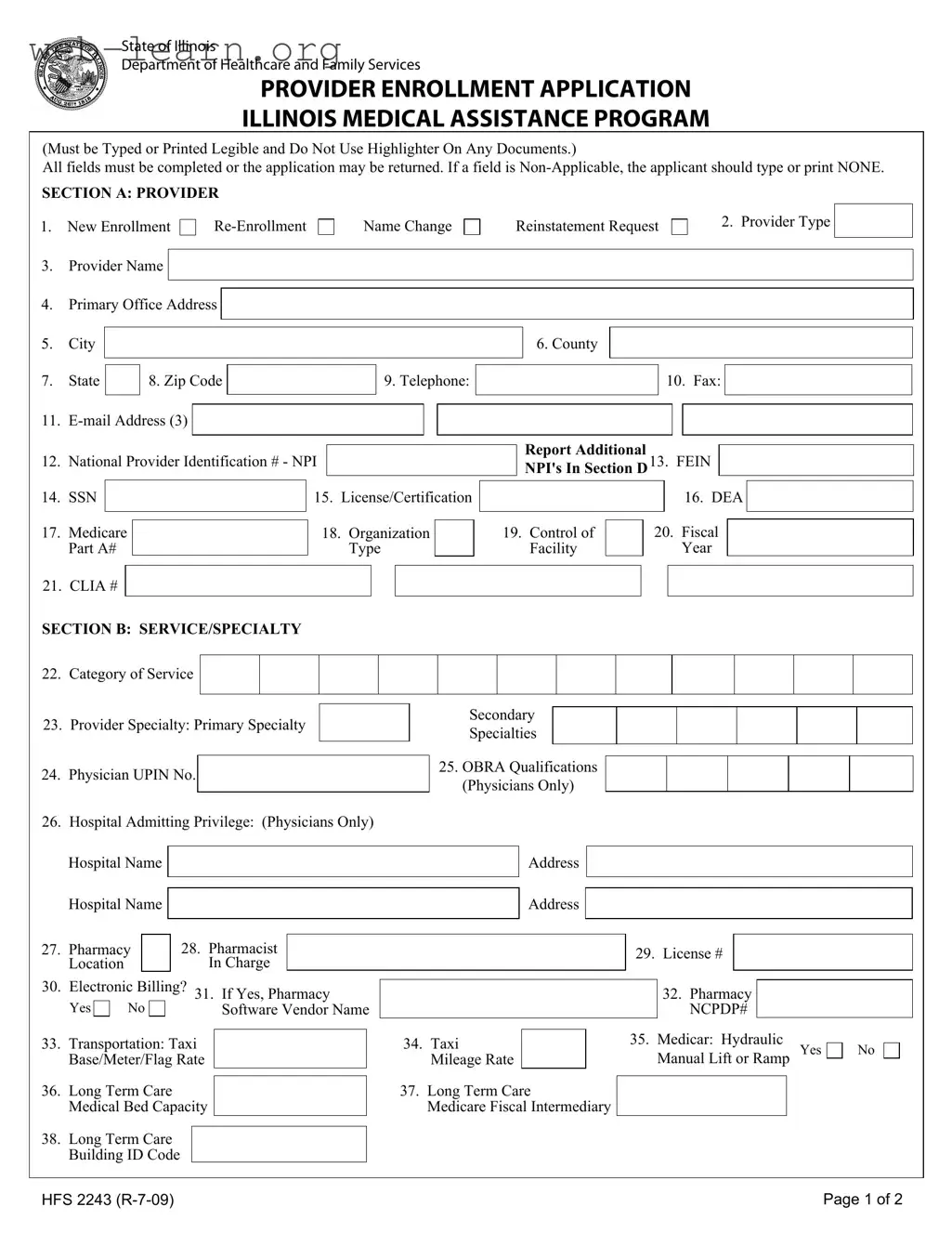
PROVIDER ENROLLMENT APPLICATION
ILLINOIS MEDICAL ASSISTANCE PROGRAM
(Must be Typed or Printed Legible and Do Not Use Highlighter On Any Documents.)
All fields must be completed or the application may be returned. If a field is
SECTION A: PROVIDER
1.New Enrollment
3.Provider Name
Name Change
Reinstatement Request
2. Provider Type
4.Primary Office Address
5.City
6. County
7.State
8. Zip Code
9. Telephone:
10. Fax:
11. |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
12. |
National Provider Identification # - NPI |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
14. |
SSN |
|
|
|
15. |
License/Certification |
|||
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
||||
17. |
Medicare |
|
|
18. |
Organization |
|
|||
|
Part A# |
|
|
|
|
Type |
|
||
Report Additional
NPI's In Section D13. FEIN
|
|
|
16. DEA |
|
|
|
|
|
|
|
|
19. Control of |
|
20. Fiscal |
|
|
|
|
|
|
|||
Facility |
|
|
Year |
|
|
21. CLIA #
SECTION B: SERVICE/SPECIALTY
22.Category of Service
23.Provider Specialty: Primary Specialty
24.Physician UPIN No.
Secondary
Specialties
25.OBRA Qualifications (Physicians Only)
26. Hospital Admitting Privilege: (Physicians Only)
|
Hospital Name |
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hospital Name |
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
28. Pharmacist |
|
|
|
|
|
|
|
|
|
|
|
|||
27. |
Pharmacy |
|
|
|
|
|
|
|
|
29. |
License # |
|
|
|
|||
|
Location |
|
|
|
In Charge |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
30. |
Electronic Billing? 31. If Yes, Pharmacy |
|
|
|
|
|
32. Pharmacy |
|
|
||||||||
|
|
|
|
|
|
|
|||||||||||
|
Yes |
No |
|
Software Vendor Name |
|
|
|
|
|
NCPDP# |
|
|
|||||
33. |
Transportation: Taxi |
|
|
|
34. Taxi |
|
|
|
35. |
Medicar: Hydraulic |
|||||||
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
Manual Lift or Ramp Yes |
|||||||||||
|
Base/Meter/Flag Rate |
|
|
Mileage Rate |
|
|
|
|
|||||||||
36. |
Long Term Care |
|
|
|
|
37. Long Term Care |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
||||||||
|
Medical Bed Capacity |
|
|
Medicare Fiscal Intermediary |
|
|
|
|
|
|
|||||||
38.Long Term Care Building ID Code
No
HFS 2243 |
Page 1 of 2 |
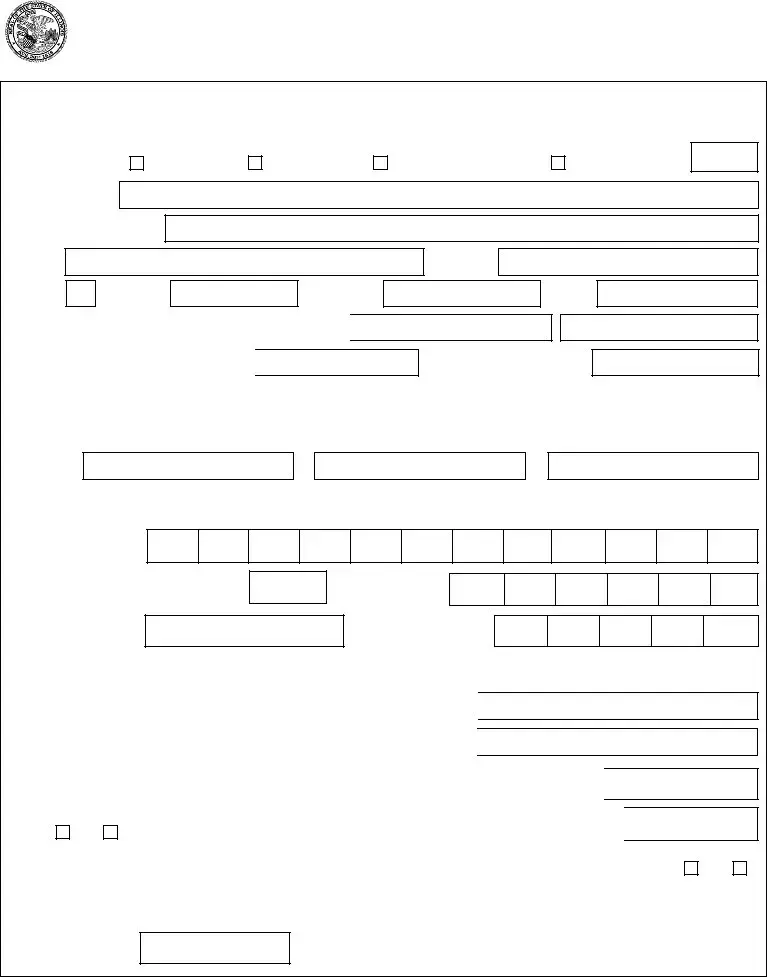
SECTION C: FORMER PARTICIPATION
39. Change of Ownership |
Yes |
40. Former Provider Number
No
Effective Date
Former Provider Name
SECTION D: ADDITIONAL NPI - National Provider Identification #
41. NPI
NPI
SECTION E: PAYEE INFORMATION
NPI
NPI
NPI
NPI
42. Name
44.DBA
45.Street Address
46.City
50.SSN/FEIN
52.Medicare Part B#
43. Telephone:
47. State |
|
|
|
48. Zip Code |
|
|
|
|
49. TIN Type Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
51. Billing Provider/Pay To NPI # |
|
|
|
|
|||
|
53. PIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
54. DMERC# |
|
|
|
|||
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
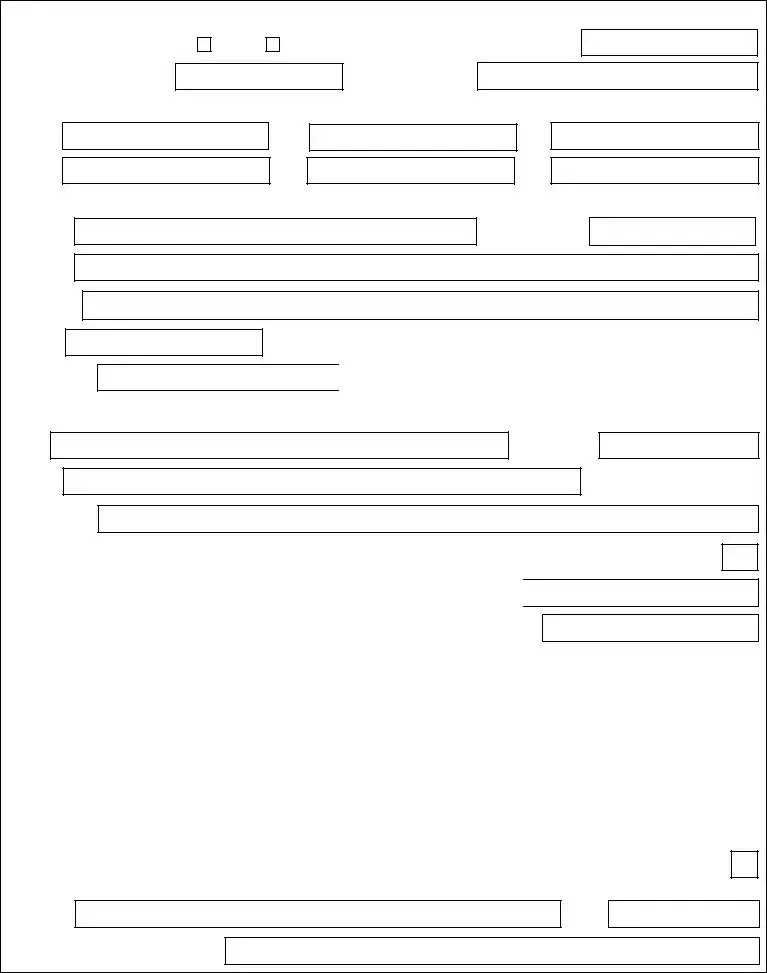
Name
DBA
Street Address
Telephone:
City |
|
|
|
|
State |
|
|
Zip Code |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
SSN/FEIN |
|
|
|
|
|
|
Billing Provider/Pay To NPI # |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|||||
Medicare Part B# |
|
PIN |
|
|
|
|
|
DMERC# |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||
SECTION F: CERTIFICATION/SIGNATURE |
|
|
|
|
|
|
|
|
|
|
|||
TIN Type Code
I understand that knowingly falsifying or willfully withholding information may be cause for the denial or termination of participation in the Medical Assistance Program and such conduct may be prosecuted under applicable Federal and State laws..
Under penalties of perjury, I hereby certify that all of the information provided in this application process is true, correct and complete and that the enrolling provider is in compliance with all applicable federal and state laws and regulations. I further certify that neither I, nor any of the following provider's employees, partners, officers, or shareholders owning at least five percent (5%) of said provider are currently barred, suspended, terminated, voluntarily withdrawn as part of a settlement agreement, or otherwise excluded from participation in the Medicaid or Medicare programs, nor are any of the above currently under sanction for, or serving a sentence for conviction of any Medicaid or Medicare program violations. I further certify that none of the above are currently sanctioned by any federal agency for any reason. I authorize the Department of Healthcare and Family Services, to verify the information provided on this application with other state and federal agencies. I further certify that I will review and comply with the Department's policies, rules and regulations including but not limited to those found at the following websites:
Illinois HFS website address: http://www.hfs.illinois.gov/
Illinois HFS Handbook updates are available: http://www.hfs.illinois.gov/handbooks
Illinois HFS Laws and Rule Regulations: http://www.hfs.illinois.gov/lawsrules/index.html
Signature:
Printed name of person signing above
Check this box if you want a provider handbook mailed
Date
HFS 2243 |
Page 2 of 2 |
| Fact Name | Detail |
|---|---|
| Form Title | Provider Enrollment Application for the Illinois Medical Assistance Program |
| Governing Law | Illinois Public Aid Code, 305 ILCS 5/1 et seq. |
| Completion Requirement | All fields must be completed; incomplete applications may be returned. |
| Non-Applicable Fields | If a field is not applicable, the applicant must type or print "NONE." |
| Provider Types | Options include New Enrollment, Re-Enrollment, Name Change, and Reinstatement Request. |
| Primary Office Address | Applicants must provide a complete primary office address, including city, county, state, and zip code. |
| National Provider Identification | Applicants must include their National Provider Identification (NPI) number. |
| Certification Requirement | Applicants must certify that all information is true and comply with applicable federal and state laws. |
| Sanction Disclosure | Applicants must disclose if they or their employees are currently barred or sanctioned from Medicaid or Medicare. |
| Electronic Billing Option | Providers must indicate if they will use electronic billing for services rendered. |
Completing the Illinois HFS 2243 form is an important step in the provider enrollment process for the Illinois Medical Assistance Program. It’s essential to ensure that every section is filled out accurately and completely to avoid delays in processing your application. Below are the steps to guide you through filling out the form.
What is the Illinois HFS 2243 form?
The Illinois HFS 2243 form is a Provider Enrollment Application for the Illinois Medical Assistance Program. It is used by healthcare providers to enroll, re-enroll, or make changes to their participation in the state's Medicaid program. This form must be completed accurately, as any incomplete sections may lead to delays or rejection of the application.
Who needs to fill out the HFS 2243 form?
This form is intended for various types of healthcare providers, including physicians, pharmacists, and long-term care facilities. If you are a new provider seeking to participate in the Illinois Medical Assistance Program or an existing provider looking to update your information, you will need to complete this form.
What information is required on the form?
The HFS 2243 form requires detailed information about the provider, including:
All fields must be completed, and if a section does not apply, the applicant should write "NONE" to avoid confusion.
What happens if I submit an incomplete form?
If the HFS 2243 form is submitted with incomplete sections, it may be returned to the applicant for corrections. This can delay the enrollment process and may affect the provider's ability to receive reimbursement for services rendered under the Illinois Medical Assistance Program. It is essential to ensure all information is accurate and complete before submission.
When filling out the Illinois HFS 2243 form, applicants often encounter various challenges that can lead to mistakes. One common error is failing to complete all required fields. Each section of the form must be filled out completely; otherwise, the application may be returned for corrections. If a particular field does not apply, it is essential to indicate this by typing or printing "NONE." Leaving fields blank can cause unnecessary delays in processing.
Another frequent mistake is using highlighters on the document. The instructions clearly state that highlighters should not be used, as they can obscure text and make it difficult for reviewers to read the information. Instead, applicants should ensure that all text is legible, whether typed or printed. This simple step can significantly improve the clarity of the application.
Inaccurate or incomplete contact information is also a common issue. Applicants often forget to provide a current telephone number, email address, or fax number. This information is crucial for communication regarding the application status. Without it, the Department of Healthcare and Family Services may struggle to reach the applicant for any necessary follow-up.
Another mistake involves the National Provider Identification (NPI) number. Some applicants either fail to include their NPI or provide an incorrect number. The NPI is a vital identifier for healthcare providers, and any errors can lead to complications in the application process. Ensuring that this number is accurate is essential for successful enrollment.
Additionally, applicants sometimes overlook the section regarding former participation in the program. Failing to disclose previous provider numbers or changes in ownership can lead to complications. Transparency in this area is critical, as it helps the reviewing agency understand the applicant's history and any potential issues that may arise.
Many applicants also neglect to check the box for receiving updates about the Illinois HFS Handbook. This oversight can result in missing important information about changes in policies or procedures that could affect their participation in the program. Staying informed is vital for compliance and successful operation within the medical assistance framework.
Moreover, some individuals fail to provide the correct tax identification number (TIN) or social security number (SSN). This information must match what is on file with the IRS. Discrepancies can lead to processing delays or even denial of the application. It is advisable to double-check these numbers before submission.
Another common error is not signing the application. The certification section requires a signature to verify that all information is accurate and complete. Without a signature, the application may be considered invalid. Applicants should remember to sign and date the form before submission.
Lastly, applicants sometimes do not review the entire form for accuracy and completeness before sending it in. A thorough review can catch mistakes that may have been overlooked during the initial filling out of the form. Taking the time to carefully check each section can prevent unnecessary delays and ensure a smoother application process.
The Illinois HFS 2243 form is a crucial document for providers seeking enrollment in the Illinois Medical Assistance Program. Alongside this form, several other documents are often required to ensure a complete application process. Below is a list of common forms and documents that may accompany the HFS 2243.
Submitting the HFS 2243 form along with these additional documents can streamline the enrollment process. Ensuring that all forms are accurate and complete will help prevent delays and facilitate a smoother transition into the Illinois Medical Assistance Program.
The Illinois HFS 2243 form serves as a provider enrollment application for the Illinois Medical Assistance Program. Several other documents share similarities with this form, primarily in their purpose and content structure. Below is a list of eight documents that are comparable to the HFS 2243 form:
When completing the Illinois HFS 2243 form, attention to detail is crucial. Below is a list of essential dos and don'ts to guide you through the process.
Following these guidelines will help ensure a smooth application process and minimize the risk of delays or rejections.
Misconceptions about the Illinois HFS 2243 form can lead to confusion and potential delays in the enrollment process. Below are four common misconceptions clarified.
When filling out the Illinois HFS 2243 form, it is crucial to ensure accuracy and completeness. Here are five key takeaways to guide you through the process:
Taking these steps seriously can enhance your chances of a smooth application process. Ensure that you review the form carefully before submission.