The Illinois Child Health Examination form plays a crucial role in ensuring the health and well-being of children enrolled in licensed child care facilities. This comprehensive document collects essential information about a child's medical history, immunizations, and physical examination results. It requires details such as the child's name, birth date, and school information, as well as a thorough health history completed by a parent or guardian. Immunization records must be verified by a healthcare provider, who also signs to confirm the accuracy of the information provided. The form includes sections for vision and hearing screenings, health concerns, and any allergies or medications the child may be taking. Additionally, it addresses physical examination requirements, including height, weight, and blood pressure, alongside assessments for potential health risks. By gathering this information, the form helps ensure that children receive the necessary support and accommodations for their health needs in educational settings.
State of Illinois
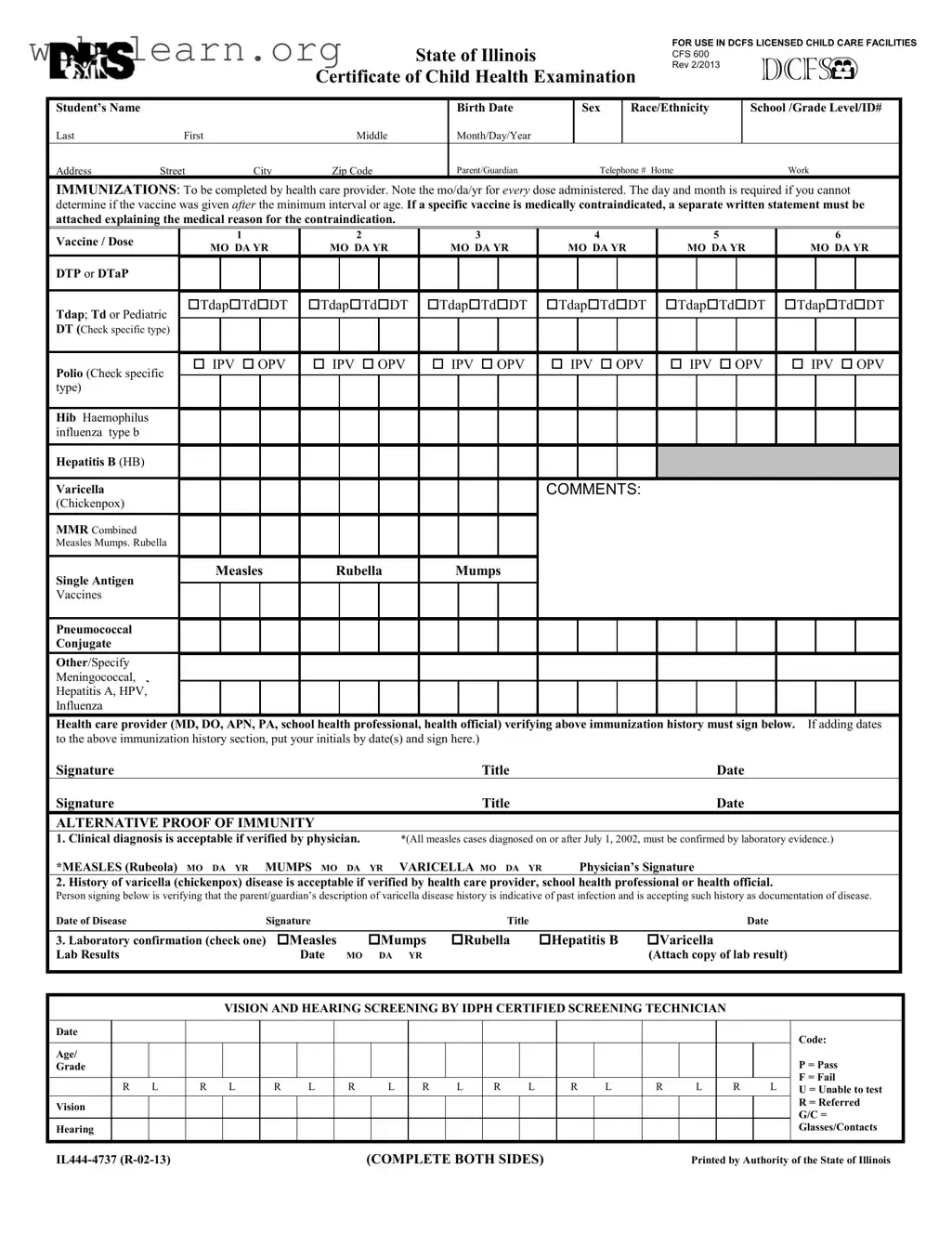
Certificate of Child Health Examination
FOR USE IN DCFS LICENSED CHILD CARE FACILITIES
CFS 600
REV 2/2013
Student’s Name
Last |
First |
Middle |
Birth Date
Month/Day/Year
Sex Race/Ethnicity
School /Grade Level/ID#
Address |
Street |
City |
Zip Code |
Parent/Guardian |
Telephone # Home |
Work |
IMMUNIZATIONS: To be completed by health care provider. Note the mo/da/yr for every dose administered. The day and month is required if you cannot determine if the vaccine was given after the minimum interval or age. If a specific vaccine is medically contraindicated, a separate written statement must be attached explaining the medical reason for the contraindication.
Vaccine / Dose |
1 |
|
2 |
|
3 |
|
4 |
|
5 |
|
6 |
|
||||||||
MO DA YR |
MO DA YR |
MO DA YR |
MO DA YR |
MO DA YR |
MO DA YR |
|||||||||||||||
|
|
|||||||||||||||||||
DTP or DTaP |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Tdap; Td or Pediatric |
TdapTdDT |
TdapTdDT |
TdapTdDT |
TdapTdDT |
TdapTdDT |
TdapTdDT |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DT (Check specific type) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Polio (Check specific |
IPV OPV |
IPV OPV |
IPV OPV |
IPV OPV |
IPV OPV |
IPV OPV |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
type) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hib Haemophilus |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
influenza type b |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hepatitis B (HB) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Varicella |
|
|
|
|
|
|
|
|
COMMENTS: |
|
|
|
|
|
|
|
|||
(Chickenpox) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MMR Combined |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Measles Mumps. Rubella |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Single Antigen |
Measles |
Rubella |
Mumps |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vaccines |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pneumococcal
Conjugate
Other/Specify |
Meningococcal, |
Hepatitis A, HPV, |
Influenza |
Health care provider (MD, DO, APN, PA, school health professional, health official) verifying above immunization history must sign below. If adding dates
to the above immunization history section, put your initials by date(s) and sign here.)
Signature |
Title |
Date |
Signature |
Title |
Date |
ALTERNATIVE PROOF OF IMMUNITY
1.Clinical diagnosis is acceptable if verified by physician. *(All measles cases diagnosed on or after July 1, 2002, must be confirmed by laboratory evidence.)
*MEASLES (Rubeola) MO DA YR MUMPS MO DA YR VARICELLA MO DA YR Physician’s Signature
2. History of varicella (chickenpox) disease is acceptable if verified by health care provider, school health professional or health official.
Person signing below is verifying that the parent/guardian’s description of varicella disease history is indicative of past infection and is accepting such history as documentation of disease.
Date of Disease |
Signature |
|
Title |
|
Date |
|
|
|
|
|
|
3. Laboratory confirmation (check one) |
Measles |
Mumps |
Rubella |
Hepatitis B |
Varicella |
Lab Results |
Date |
MO DA YR |
|
|
(Attach copy of lab result) |
VISION AND HEARING SCREENING BY IDPH CERTIFIED SCREENING TECHNICIAN
Date
Age/
Grade
R |
L |
R |
L |
R |
L |
R |
L |
R |
L |
R |
L |
R |
L |
R |
L |
R |
L |
Vision
Hearing
Code:
P = Pass
F = Fail
U = Unable to test R = Referred G/C = Glasses/Contacts
(COMPLETE BOTH SIDES) |
Printed by Authority of the State of Illinois |
Last |
First |
Middle |
|
|
|
|
|
Birth Date
Month/Day/ Year
Sex School
Grade Level/ ID
|
HEALTH HISTORY |
TO BE COMPLETED AND SIGNED BY PARENT/GUARDIAN AND VERIFIED BY HEALTH CARE PROVIDER |
||||||||||
|
|
|
|
|
|
|
|
|
||||
|
ALLERGIES (Food, drug, insect, other) |
|
|
|
|
MEDICATION (List all prescribed or taken on a regular basis.) |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Diagnosis of asthma? |
|
Yes |
No |
|
|
Loss of function of one of paired |
|
Yes |
No |
|
|
|
Child wakes during night coughing? |
Yes |
No |
|
|
organs? (eye/ear/kidney/testicle) |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Birth defects? |
|
Yes |
No |
|
|
Hospitalizations? |
|
Yes |
No |
|
|
|
|
|
|
|
|
|
When? What for? |
|
|
|
|
|
|
Developmental delay? |
|
Yes |
No |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Blood disorders? Hemophilia, |
|
Yes |
No |
|
|
Surgery? (List all.) |
|
Yes |
No |
|
|
|
Sickle Cell, Other? Explain. |
|
|
|
|
|
When? What for? |
|
|
|
|
|
|
Diabetes? |
|
Yes |
No |
|
|
Serious injury or illness? |
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Head injury/Concussion/Passed out? |
Yes |
No |
|
|
TB skin test positive (past/present)? |
|
Yes* |
No |
*If yes, refer to local health |
||
|
|
|
|
|
|
|
|
|
|
|
department. |
|
|
Seizures? What are they like? |
|
Yes |
No |
|
|
TB disease (past or present)? |
|
Yes* |
No |
||
|
|
|
|
|
|
|
|
|
|
|
||
|
Heart problem/Shortness of breath? |
Yes |
No |
|
|
Tobacco use (type, frequency)? |
|
Yes |
No |
|
||
|
|
|
|
|
|
|
|
|
|
|
||
|
Heart murmur/High blood pressure? |
Yes |
No |
|
|
Alcohol/Drug use? |
|
Yes |
No |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dizziness or chest pain with |
|
Yes |
No |
|
|
Family history of sudden death |
|
Yes |
No |
|
|
|
exercise? |
|
|
|
|
|
before age 50? (Cause?) |
|
|
|
|
|
|
Eye/Vision problems? _____ |
Glasses Contacts Last exam by eye doctor ______ |
Dental |
Braces Bridge |
Plate |
Other |
||||||
|
Other concerns? (crossed eye, drooping lids, squinting, difficulty reading) |
|
|
|
|
|
|
|||||
|
Ear/Hearing problems? |
|
Yes |
No |
|
|
Information may be shared with appropriate personnel for health and educational purposes. |
|||||
|
|
|
|
|
|
|
Parent/Guardian |
|
|
|
|
|
|
Bone/Joint problem/injury/scoliosis? |
Yes |
No |
|
|
|
|
|
|
|||
|
|
|
Signature |
|
|
|
|
Date |
||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|||||
|
PHYSICAL EXAMINATION REQUIREMENTS |
Entire section below to be completed by MD/DO/APN/PA |
|
|
||||||||
|
HEAD CIRCUMFERENCE if < |
|
|
HEIGHT |
WEIGHT |
|
BMI |
|
B/P |
|||
|
|
|
|
|
||||||||
|
DIABETES SCREENING (NOT REQUIRED FOR DAY CARE) |
BMI>85% age/sex Yes |
No |
And any two of the following: Family History Yes No |
||||||||
Ethnic Minority Yes No Signs of Insulin Resistance (hypertension, dyslipidemia, polycystic ovarian syndrome, acanthosis nigricans) Yes No At Risk Yes No
LEAD RISK QUESTIONNAIRE Required for children age 6 months through 6 years enrolled in licensed or public school operated day care, preschool, nursery school and/or kindergarten. (Blood test required if resides in Chicago or high risk zip code.)
Questionnaire Administered ? Yes No Blood Test Indicated? Yes No |
Blood Test Date |
Result |
TB SKIN OR BLOOD TEST Recommended only for children in
in high prevalence countries or those exposed to adults in |
No test needed |
Test performed |
|
|
|||||||||
Skin Test: |
Date Read |
/ |
/ |
Result: Positive |
Negative |
mm ______________ |
|
|
|||||
Blood Test: |
Date Reported |
/ |
/ |
Result: Positive |
Negative |
Value ______________ |
|
|
|||||
LAB TESTS (Recommended) |
|
Date |
|
Results |
|
|
|
Date |
|
Results |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hemoglobin or Hematocrit |
|
|
|
|
|
Sickle Cell (when indicated) |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Urinalysis |
|
|
|
|
|
|
|
Developmental Screening Tool |
|
|
|
||
SYSTEM REVIEW |
Normal |
|
|
Normal |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Skin |
|
|
|
|
|
|
|
Endocrine |
|
|
|
|
|
Ears |
|
|
|
|
|
|
|
Gastrointestinal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Eyes |
|
|
|
|
|
Amblyopia |
Yes No |
|
|
|
LMP |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Nose |
|
|
|
|
|
|
|
Neurological |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Throat |
|
|
|
|
|
|
|
Musculoskeletal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mouth/Dental |
|
|
|
|
|
|
|
Spinal Exam |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cardiovascular/HTN |
|
|
|
|
|
|
Nutritional status |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Respiratory |
|
|
|
|
|
Diagnosis of Asthma |
Mental Health |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Currently Prescribed Asthma Medication: |
|
|
|
|
|
|
|
|
|
||||
|
medication (e.g. Short Acting Beta Agonist) |
|
Other |
|
|
|
|
|
|||||
Controller medication (e.g. inhaled corticosteroid) |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|||||||
NEEDS/MODIFICATIONS required in the school setting |
|
DIETARY Needs/Restrictions |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SPECIAL INSTRUCTIONS/DEVICES e.g. safety glasses, glass eye, chest protector for arrhythmia, pacemaker, prosthetic device, dental bridge, false teeth, athletic support/cup
MENTAL HEALTH/OTHER Is there anything else the school should know about this student?
If you would like to discuss this student’s health with school or school health personnel, check title: Nurse Teacher Counselor Principal
EMERGENCY ACTION needed while at school due to child’s health condition (e.g. ,seizures, asthma, insect sting, food, peanut allergy, bleeding problem, diabetes, heart problem)? Yes No If yes, please describe.
On the basis of the examination on this day, I approve this child’s participation in |
|
(If No or Modified please attach explanation.) |
|
||
PHYSICAL EDUCATION |
Yes No Modified |
INTERSCHOLASTIC SPORTS |
Yes |
No Limited |
|
Print Name |
(MD,DO, APN, PA) |
Signature |
|
Date |
|
Address |
|
|
Phone |
|
|
|
|
|
|
|
|
(Complete Both Sides)
| Fact Name | Details |
|---|---|
| Purpose | The Illinois Child Health Examination form is designed to ensure that children in licensed child care facilities receive necessary health screenings and vaccinations. |
| Governing Law | The form is governed by the Illinois School Code, specifically 105 ILCS 5/27-8.1, which mandates health examinations for children entering school. |
| Immunization Records | Healthcare providers must complete the immunization section, noting the date for each vaccine dose administered. |
| Alternative Proof of Immunity | Parents can provide alternative proof of immunity through clinical diagnosis, history of disease, or laboratory confirmation, as specified on the form. |
| Vision and Hearing Screening | Screening for vision and hearing must be conducted by certified technicians, with results documented on the form. |
| Health History Section | Parents or guardians must fill out a comprehensive health history, including allergies, medications, and any significant medical conditions. |
| Physical Examination | A physical examination must be completed by a licensed healthcare provider, including height, weight, and blood pressure measurements. |
| Lead Risk Questionnaire | Children aged 6 months to 6 years must undergo a lead risk questionnaire, with blood tests required for those in high-risk areas. |
| Emergency Action Plans | The form allows for the inclusion of emergency action plans for children with specific health conditions, ensuring safety at school. |
| Signature Requirement | The form must be signed by both the healthcare provider and the parent or guardian to verify the information provided. |
Filling out the Illinois Child Health Examination form is essential for ensuring that your child meets health requirements for school and childcare. It’s a straightforward process, but attention to detail is important. Follow these steps to complete the form accurately.
What is the purpose of the Illinois Child Health Examination form?
The Illinois Child Health Examination form is designed to ensure that children in licensed childcare facilities receive necessary health assessments. It collects vital information regarding a child's health history, immunizations, and results from vision and hearing screenings. This form helps healthcare providers, parents, and schools work together to promote the health and well-being of children.
Who is responsible for completing the form?
The form must be completed by both a parent or guardian and a qualified healthcare provider. Parents or guardians are required to provide detailed health history and any allergies or medications the child may be taking. The healthcare provider, such as a physician or nurse practitioner, must verify the child's immunization records and conduct necessary physical examinations. This collaborative effort ensures accurate and comprehensive health information is documented.
What immunizations need to be documented on the form?
The form requires documentation of several key immunizations, including:
If a specific vaccine is medically contraindicated, a separate written statement must be attached to explain the reason. This ensures that the child's health needs are accurately documented and addressed.
What should parents do if their child has a health condition?
If a child has any health conditions, such as asthma, diabetes, or allergies, it is crucial for parents to provide detailed information on the form. This includes any medications the child is taking and any necessary modifications or emergency actions required while at school. By sharing this information, parents help ensure that school personnel are aware of the child's health needs and can respond appropriately in case of an emergency.
Filling out the Illinois Child Health Examination form can be a straightforward process, but there are common mistakes that can lead to delays or complications. One frequent error occurs when parents forget to include the child's full name. It is crucial to provide the last, first, and middle names clearly. This ensures that the child's records are accurate and easily accessible.
Another common mistake is not providing the correct birth date. Parents often write the date in a format that can be confusing. Always use the month/day/year format to avoid misunderstandings. An incorrect birth date can complicate the child's health records and may lead to issues with school enrollment.
Immunization records are essential for this form. A mistake many make is failing to include the exact dates for each vaccine. It is important to note the month, day, and year for every dose administered. If a vaccine is medically contraindicated, a separate statement explaining the reason must be attached. Omitting this information can delay the processing of the form.
Parents sometimes overlook the section for allergies and medications. This part must be completed thoroughly. Leaving it blank or providing vague answers can lead to serious health risks for the child. Always list all allergies and medications the child is currently taking to ensure proper care.
Another mistake involves the health history section. Parents may skip questions or provide incomplete answers. Each question is designed to gather important information about the child's health. Providing accurate and detailed responses helps healthcare providers understand the child's needs better.
Additionally, signatures are often forgotten. The form requires signatures from both the parent or guardian and the healthcare provider. Without these signatures, the form may be deemed invalid. Ensure that all necessary parties sign the form before submission.
Lastly, some parents may not review the entire form before submitting it. Taking a moment to double-check all entries can prevent many of the issues mentioned above. A thorough review ensures that all information is accurate and complete, facilitating a smoother process for the child's health examination.
When preparing for the health and educational needs of children, various forms accompany the Illinois Child Health Examination form. Each document serves a specific purpose in ensuring comprehensive health oversight and compliance with state regulations. Below is a list of commonly used forms that work in conjunction with the Illinois Child Health Examination form.
Each of these documents plays a significant role in safeguarding children's health and well-being in educational settings. Proper completion and submission of these forms can help ensure that children receive the necessary support and care they need to thrive.
School Health Assessment Form: Similar to the Illinois Child Health Examination form, this document collects health information, immunization records, and physical assessments for students entering school. It ensures that children meet health requirements for educational participation.
Wellness Checkup Form: This form serves a similar purpose by documenting a child's overall health status, including immunizations, medical history, and any health concerns. Both forms aim to provide a comprehensive view of a child's health for educational settings.
Immunization Record: Like the Illinois Child Health Examination form, this document focuses specifically on immunization history. It tracks vaccinations received and ensures compliance with state health regulations for school attendance.
Physical Examination Report: This report details the findings from a child's physical exam, including height, weight, and any health issues identified. It complements the Illinois Child Health Examination form by providing a thorough assessment of a child's physical health.
Sports Physical Form: This document is required for children participating in sports. It assesses a child's fitness and health status, similar to the physical examination section of the Illinois Child Health Examination form, ensuring safety during athletic activities.
Health History Questionnaire: Parents fill out this form to provide detailed information about their child's medical history, allergies, and past illnesses. This aligns with the health history section of the Illinois Child Health Examination form.
Lead Risk Assessment Questionnaire: This form is used to evaluate a child's risk for lead exposure, similar to the lead risk questionnaire in the Illinois Child Health Examination form. It is crucial for identifying children who may need further testing.
Emergency Care Plan: This document outlines specific health needs and emergency procedures for children with chronic conditions. It complements the Illinois Child Health Examination form by providing actionable information for school staff.
Medication Administration Form: This form allows parents to authorize school personnel to administer medication to their child. It is similar in purpose to the Illinois Child Health Examination form, which may include information about prescribed medications.
Developmental Screening Form: This document assesses a child's developmental milestones and health status. It parallels the developmental screening tool section of the Illinois Child Health Examination form, ensuring comprehensive health evaluations.
When filling out the Illinois Child Health Examination form, there are important guidelines to follow. Here’s a list of things you should and shouldn't do:
Understanding the Illinois Child Health Examination form can be challenging due to various misconceptions. Here are some common misunderstandings explained:
By addressing these misconceptions, parents and guardians can better navigate the requirements of the Illinois Child Health Examination form, ensuring their child's health needs are met appropriately.
Ensure accurate information by filling out the Illinois Child Health Examination form completely. This includes providing the child's name, birth date, sex, race/ethnicity, and school details.
Immunization records must be filled out by a qualified health care provider. Each vaccine administered should be documented with the corresponding date, and if a vaccine is medically contraindicated, a written explanation is required.
Parents or guardians need to complete the health history section. This includes important details about allergies, medications, and any significant medical conditions or past hospitalizations.
The physical examination section must be completed by a licensed health care professional. This includes measurements such as height, weight, and blood pressure, along with any necessary lab tests.
Keep a copy of the completed form for your records. It may be needed for future reference in school or health-related situations.