The Hospital Bill form is an essential document that provides a comprehensive overview of the services rendered during a patient's visit to the hospital. This form outlines crucial details such as the patient's name, account number, and date of service, ensuring that all relevant information is easily accessible. It includes a breakdown of charges, showing individual costs for services like emergency room visits and pharmacy expenses, as well as total charges, payments, and adjustments. Payment instructions are clearly stated, emphasizing the urgency of settling the amount due upon receipt. For those paying by credit card, the form offers a section to fill out card details securely. Additionally, it encourages patients to update their personal and insurance information, promoting accuracy in billing. The form also provides contact information for Patient Financial Services, allowing patients to seek assistance or request an itemized statement if needed. Overall, the Hospital Bill form serves as a vital tool for managing medical expenses and ensuring transparency in healthcare billing.
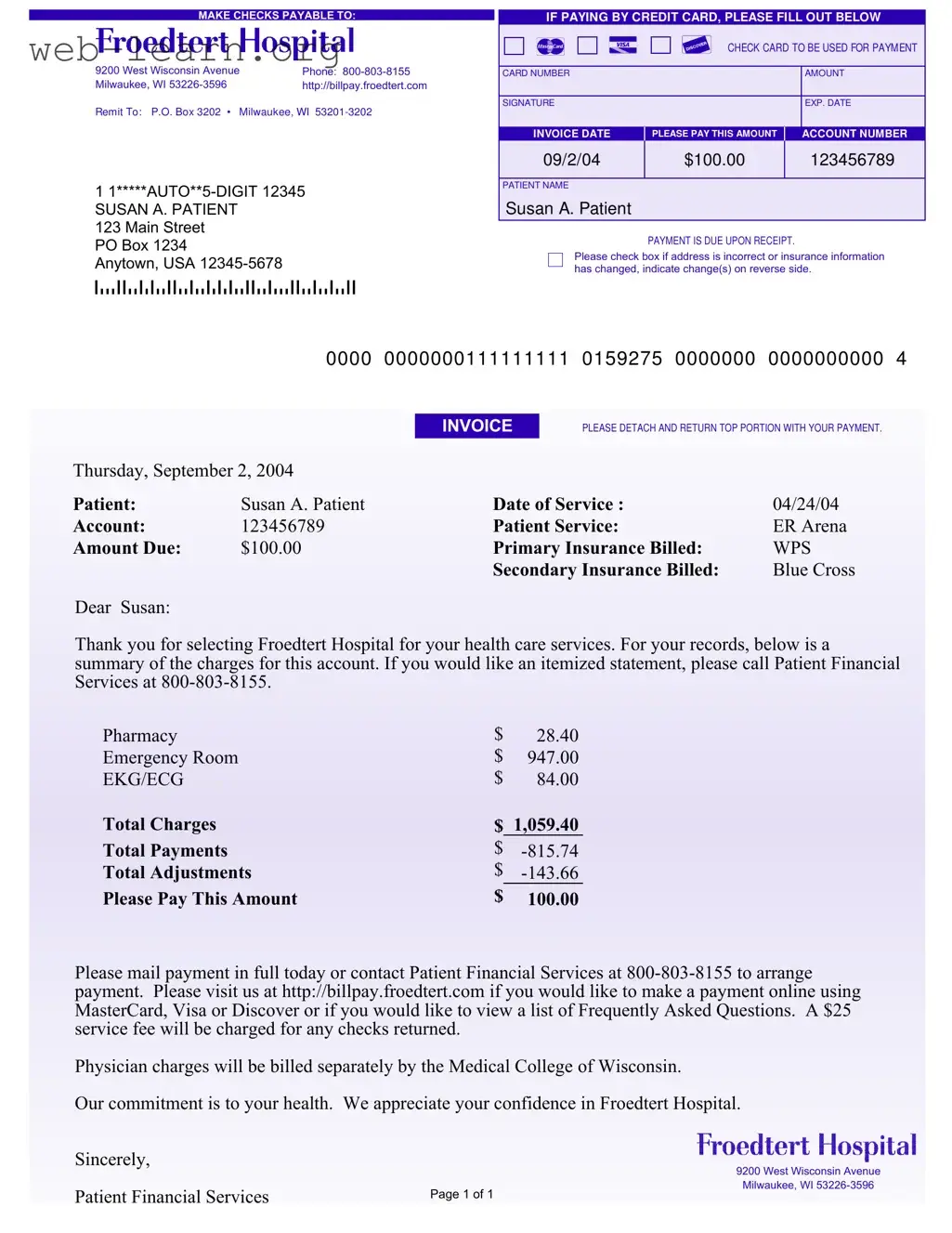
MAKE CHECKS PAYABLE TO:
9200 West Wisconsin Avenue |
Phone: |
Milwaukee, WI |
http://billpay.froedtert.com |
Remit To: P.O. Box 3202 • Milwaukee, WI
1
SUSAN A. PATIENT
123 Main Street
PO Box 1234
Anytown, USA
IF PAYING BY CREDIT CARD, PLEASE FILL OUT BELOW
CHECK CARD TO BE USED FOR PAYM ENT
CARD NUMBER |
AMOUNT |
|
|
SIGNATURE |
EXP. DATE |
|
|
INVOICE DATE |
PLEASE PAY THIS AMOUNT |
ACCOUNT NUMBER |
09/2/04 |
$100.00 |
123456789 |
|
|
|
PATIENT NAME
Susan A. Patient
PAYMENT IS DUE UPON RECEIPT.
Please check box if address is incorrect or insurance information has changed, indicate change(s) on reverse side.
|
0000 |
0000000111111111 |
0159275 |
0000000 |
0000000000 |
4 |
|
|
INVOICE |
PLEASE DETACH AND RETURN TOP PORTION WITH YOUR PAYMENT. |
|
||
Thursday, September 2, 2004 |
|
|
|
|
|
|
Patient: |
Susan A. Patient |
Date of Service : |
|
04/24/04 |
|
|
Account: |
123456789 |
Patient Service: |
|
ER Arena |
|
|
Amount Due: |
$100.00 |
Primary Insurance Billed: |
WPS |
|
||
|
|
Secondary Insurance Billed: |
Blue Cross |
|
||
Dear Susan:
Thank you for selecting Froedtert Hospital for your health care services. For your records, below is a summary of the charges for this account. If you would like an itemized statement, please call Patient Financial Services at
Pharmacy |
$ |
28.40 |
Emergency Room |
$ |
947.00 |
EKG/ECG |
$ |
84.00 |
Total Charges |
$ |
1,059.40 |
Total Payments |
$ |
|
Total Adjustments |
$ |
|
Please Pay This Amount |
$ |
100.00 |
Please mail payment in full today or contact Patient Financial Services at
Physician charges will be billed separately by the Medical College of Wisconsin.
Our commitment is to your health. We appreciate your confidence in Froedtert Hospital.
Sincerely,
9200 West Wisconsin Avenue
|
Milwaukee, WI |
Patient Financial Services |
Page 1 of 1 |
|
PLEASE UPDATE ANY INFORM ATION THAT HAS CHANGED SINCE YOUR LAST STATEM ENT
ABOUT YOU:
YOUR NAME (Last, First, Middle Initial)
ADDRESS
CITY |
|
|
|
|
|
|
|
|
|
|
STATE |
|
|
|
|
ZIP |
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE |
|
|
|
|
|
|
|
|
|
MARITAL STATUS |
|
|
|
|
Separated |
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Single |
|
|
|
|
Divorced |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Married |
|
|
|
|
Widowed |
|
||||||
EMPLOYER'S NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMPLOYER'S ADDRESS |
|
|
|
|
|
|
|
CITY |
STATE |
|
|
|
|
ZIP |
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ABOUT YOUR INSURANCE:
YOUR PRIMARY INSURANCE COMPANY'S NAME
PRIMARY INSURANCE COMPANY'S ADDRESS
CITY |
STATE |
ZIP |
||
|
|
|
|
|
POLICYHOLDER'S ID NUMBER |
GROUP PLAN NUMBER |
|
|
|
|
|
|
|
|
YOUR SECONDARY INSURANCE COMPANY'S NAME |
|
|
|
|
|
|
|
|
|
SECONDARY INSURANCE COMPANY'S ADDRESS |
|
|
|
|
|
|
|
|
|
CITY |
STATE |
ZIP |
||
|
|
|
|
|
POLICYHOLDER'S ID NUMBER |
GROUP PLAN NUMBER |
|
|
|
|
|
|
|
|
| Fact Name | Description |
|---|---|
| Payee Information | Checks should be made payable to Froedtert Hospital, located at 9200 West Wisconsin Avenue, Milwaukee, WI 53226-3596. |
| Contact Information | For inquiries, patients can call Patient Financial Services at 800-803-8155. |
| Payment Due Date | Payment is due upon receipt of the bill. |
| Payment Options | Payments can be made by check or credit card. Online payments are also accepted via http://billpay.froedtert.com. |
| Invoice Details | The invoice includes details like the date of service, account number, and total amount due, which is $100.00. |
| Insurance Information | Primary and secondary insurance companies are billed directly. Patients should update any changes in their insurance information. |
| Itemized Statement | Patients can request an itemized statement by contacting Patient Financial Services. |
| Returned Check Fee | A $25 service fee will be charged for any checks returned due to insufficient funds. |
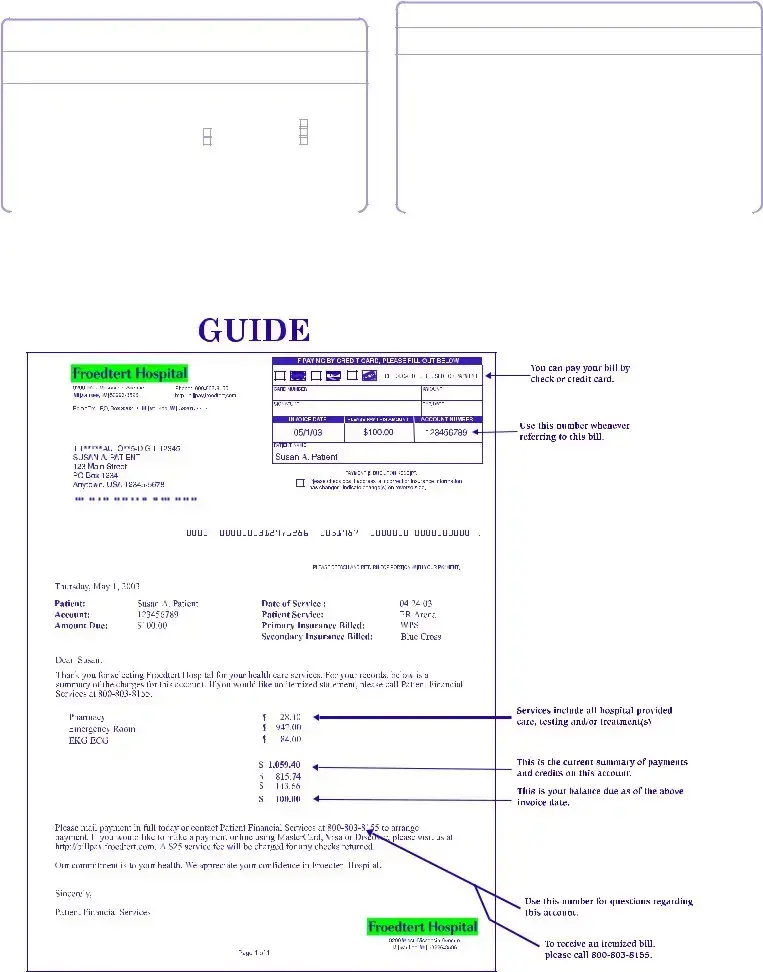
Completing the Hospital Bill form is an important step in managing your healthcare expenses. This guide will help you fill out the form accurately to ensure that your payment is processed smoothly. Follow the steps below to provide the necessary information.
Once you have completed the form, ensure that you keep a copy for your records. If you have any questions or need assistance, you can contact Patient Financial Services at the provided phone number. Your timely payment will help maintain your healthcare services smoothly.
If you receive a Hospital Bill form, it’s important to review it carefully. Check the details, such as your name, address, and the services listed. Ensure that the charges reflect the care you received. If you notice any discrepancies or if your insurance information has changed, update the information on the form and return it promptly. If everything looks correct, proceed with the payment instructions provided on the form.
You have multiple options for paying your hospital bill. You can mail a check made payable to Froedtert Hospital to the address provided on the form. If you prefer to pay by credit card, fill out the credit card section on the form, including the card number, amount, and your signature. Alternatively, you can visit http://billpay.froedtert.com to pay online using MasterCard, Visa, or Discover. Make sure to pay promptly to avoid any late fees.
If you have questions regarding your bill, you can contact Patient Financial Services at 800-803-8155. They can provide you with detailed explanations of your charges and help you understand your payment options. Additionally, you can request an itemized statement if you need more information about specific services or charges.
In the event that your payment is returned, a $25 service fee will be charged. To avoid this situation, ensure that you have sufficient funds in your account before issuing a check. If you encounter any issues with your payment, contact Patient Financial Services as soon as possible to discuss your options and avoid further complications.
When filling out the Hospital Bill form, many individuals make critical mistakes that can delay processing or lead to complications. One common error is providing incorrect personal information. This includes misspelling names, entering the wrong address, or failing to update changes in marital status. Such inaccuracies can result in billing issues and may prevent timely communication regarding the account.
Another frequent mistake is overlooking insurance details. Individuals often forget to include their primary and secondary insurance information or may neglect to update these details if they have changed. This can lead to the hospital billing the wrong insurance company, which can complicate payment and potentially leave the patient responsible for the entire amount due.
People also tend to ignore the payment instructions. It is essential to follow the guidelines provided on the form, including the payment methods accepted and the correct mailing address for payments. Failure to adhere to these instructions can lead to delays in processing payments or, worse, the payment being sent to the wrong location.
Finally, many individuals forget to sign the form. A signature is often required to authorize payment and confirm the accuracy of the information provided. Without a signature, the hospital may not process the payment, causing unnecessary stress and potential late fees for the patient.
When dealing with hospital bills, several other documents often accompany the Hospital Bill form. Understanding these forms can help patients navigate their healthcare expenses more effectively. Here’s a brief overview of some common documents you may encounter.
By familiarizing yourself with these documents, you can better manage your healthcare finances and ensure that you fully understand your billing situation. Each document serves a specific purpose, helping to clarify costs, facilitate payments, and ensure that patients receive the necessary support for their medical expenses.
Invoice: Like the Hospital Bill form, an invoice details services rendered and the amount due. It includes a breakdown of charges and payment instructions, making it easy for the recipient to understand what they owe.
Statement of Account: This document summarizes the financial activity on an account over a specific period. Similar to the Hospital Bill form, it shows charges, payments, and any outstanding balance, helping the recipient track their financial obligations.
Payment Reminder: A payment reminder serves to notify the recipient of an upcoming or overdue payment. It often mirrors the Hospital Bill form by including details about the amount due and payment methods, ensuring that the recipient is aware of their financial responsibilities.
Insurance Claim Form: This form is used to request payment from an insurance company for medical services. Like the Hospital Bill form, it contains patient information, details of services provided, and amounts billed, facilitating the claims process for both patients and insurers.
When filling out the Hospital Bill form, it’s essential to be thorough and accurate. Here are some important dos and don’ts to keep in mind:
By following these guidelines, you can help ensure that your payment process goes smoothly and that your information is correctly recorded. This will facilitate a better experience with your healthcare provider.
While the bill states that payment is due upon receipt, it is important to review the charges and verify insurance claims before making a payment.
The total amount due reflects the balance after adjustments and payments. It is crucial to understand how this amount was calculated.
Patients have the right to question any charges. If there are discrepancies, contacting Patient Financial Services is advisable.
Insurance coverage varies. Patients should verify what their insurance plan covers and what their financial responsibility will be.
The bill provides options for payment via credit card online. Patients can use MasterCard, Visa, or Discover for convenience.
Some charges, like physician fees, may be billed separately. It is essential to understand that additional bills may arrive.
Patients must actively update their information on the bill. This includes any changes to personal or insurance details.
Even with insurance, patients are responsible for understanding their bills and ensuring that their insurance processes claims correctly.
Late payments may result in additional fees, such as a service charge for returned checks. Timely payment is encouraged to avoid extra costs.
When handling the Hospital Bill form, keep these important points in mind: