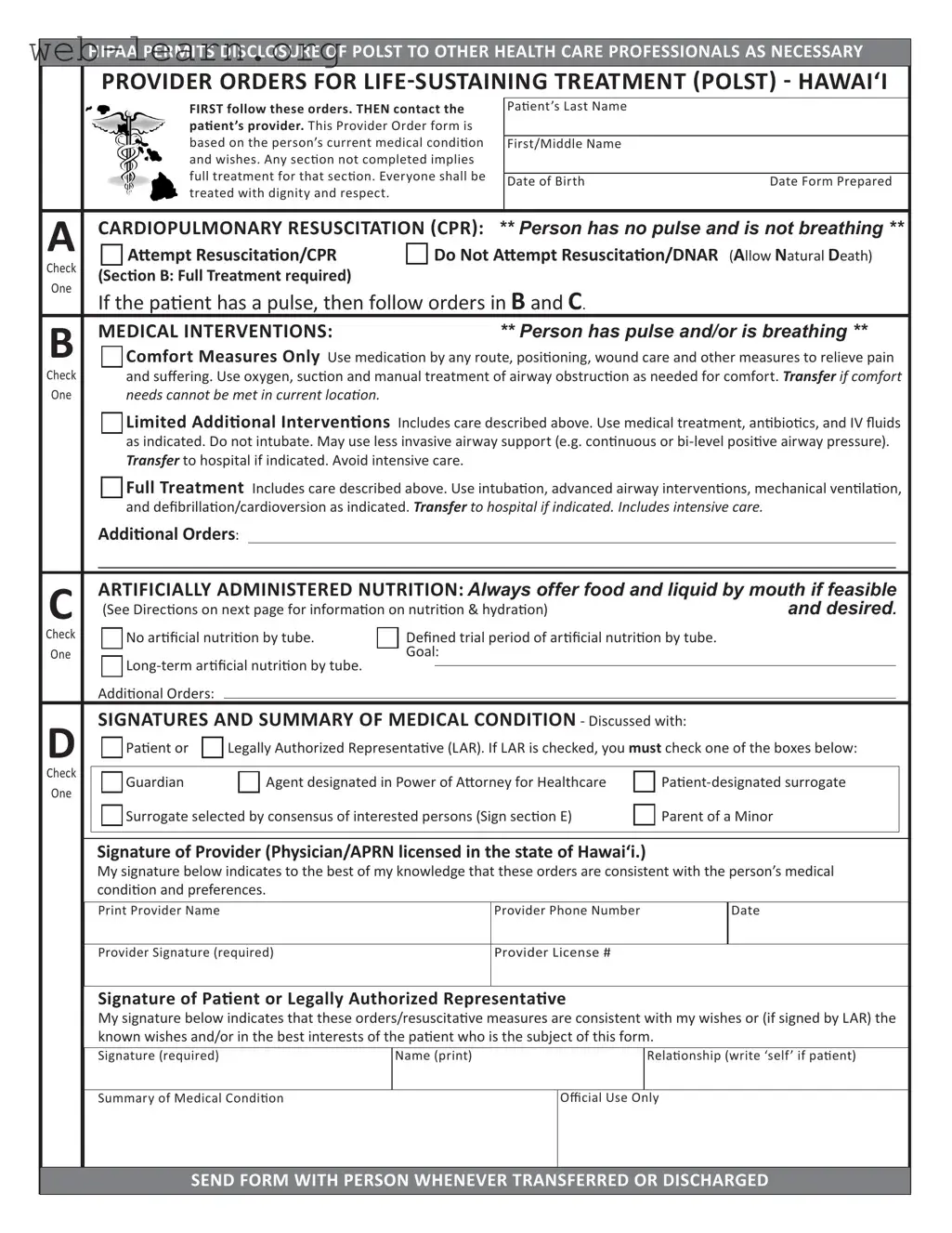
The Hawaii Provider Orders for Life-Sustaining Treatment (POLST) form is an essential tool designed to ensure that individuals receive medical care aligned with their personal preferences, especially during critical health situations. This form outlines specific medical orders regarding resuscitation, medical interventions, and nutrition, providing clear guidance for healthcare professionals. It emphasizes the importance of dignity and respect in patient care, ensuring that each person's wishes are honored. The POLST form includes sections for cardiopulmonary resuscitation (CPR) preferences, medical interventions ranging from comfort measures to full treatment, and decisions about artificially administered nutrition. Additionally, it requires signatures from both a healthcare provider and the patient or their legally authorized representative, confirming that the orders reflect the patient's medical condition and desires. Healthcare providers must adhere to the directives outlined in the POLST form, which can be modified or revoked as the patient's health status or preferences change. Regular reviews of the POLST form are recommended to ensure it remains consistent with the patient's current wishes and medical condition.
HIPAA PERMITS DISCLOSURE OF POLST TO OTHER HEALTH CARE PROFESSIONALS AS NECESSARY
PROVIDER ORDERS FOR
|
FIRST follow these orders. THEN contact the |
|
Paient’s Last Name |
|
|
|
paient’s provider. This Provider Order form is |
|
|
|
|
|
based on the person’s current medical condiion |
|
|
|
|
|
|
First/Middle Name |
|
||
|
and wishes. Any secion not completed implies |
|
|
|
|
|
full treatment for that secion. Everyone shall be |
|
|
|
|
|
|
Date of Birth |
Date Form Prepared |
||
|
treated with dignity and respect. |
|
|
||
|
|
|
|
|
|
|
|
|
|||
A |
CARDIOPULMONARY RESUSCITATION (CPR): ** Person has no pulse and is not breathing ** |
||||
Atempt Resuscitaion/CPR |
Do Not Atempt Resuscitaion/DNAR (Allow Natural Death) |
||||
Check |
(Secion B: Full Treatment required) |
|
|
|
|
One |
|
|
|
|
|
If the paient has a pulse, then follow orders in B and C. |
|
||||
|
|
||||
B |
MEDICAL INTERVENTIONS: |
|
** Person has pulse and/or is breathing ** |
||
Comfort Measures Only Use medicaion by any route, posiioning, wound care and other measures to relieve pain |
|||||
Check |
and suffering. Use oxygen, sucion and manual treatment of airway obstrucion as needed for comfort. TRANSFER IF COMFORT |
||||
One |
needs cannot be met in current locaion. |
|
|
|
|
Limited Addiional Intervenions Includes care described above. Use medical treatment, anibioics, and IV fluids as indicated. Do not intubate. May use less invasive airway support (e.g. coninuous or
Full Treatment Includes care described above. Use intubaion, advanced airway intervenions, mechanical venilaion, and defibrillaion/cardioversion as indicated. TRANSFER to hospital if indicated. Includes intensive care.
Addiional Orders:
C |
ARTIFICIALLY ADMINISTERED NUTRITION: Always offer food and liquid by mouth if feasible |
|
|||||
(See Direcions on next page for informaion on nutriion & hydraion) |
and desired. |
|
|||||
Check |
No arificial nutriion by tube. |
Defined trial period of arificial nutriion by tube. |
|
||||
One |
Goal: |
|
|
|
|||
|
|
|
|
|
|
||
|
|
|
|
|
|
||
|
Addiional Orders: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D |
SIGNATURES AND SUMMARY OF MEDICAL CONDITION - Discussed with: |
|
|||||
Paient or |
Legally Authorized Representaive (LAR). If LAR is checked, you must check one of the boxes below: |
|
|||||
|
|
||||||
Check |
|
|
|
|
|
|
|
Guardian |
Agent designated in Power of Atorney for Healthcare |
|
|||||
One |
|
||||||
|
|
|
|
|
|
|
|
|
Surrogate selected by consensus of interested persons (Sign secion E) |
Parent of a Minor |
|
||||
|
|
|
|
|
|
|
|
Signature of Provider (Physician/APRN licensed in the state of Hawai‘i.)
My signature below indicates to the best of my knowledge that these orders are consistent with the person’s medical condiion and preferences.
Print Provider Name |
Provider Phone Number |
Date |
|
|
|
Provider Signature (required) |
Provider License # |
|
Signature of Paient or Legally Authorized Representaive
My signature below indicates that these orders/resuscitaive measures are consistent with my wishes or (if signed by LAR) the known wishes and/or in the best interests of the paient who is the subject of this form.
Signature (required) |
Name (print) |
Relaionship (write ‘self’ if paient) |
Summary of Medical Condiion
Official Use Only
SEND FORM WITH PERSON WHENEVER TRANSFERRED OR DISCHARGED
HIPAA PERMITS DISCLOSURE OF POLST TO OTHER HEALTH CARE PROFESSIONALS AS NECESSARY
Paient Name (last, first, middle)
Date of Birth
Gender
M F
Patient’s Preferred Emergency Contact or Legally Authorized Representative
Name |
Address |
|
Phone Number |
|
|
|
|
Health Care Professional Preparing Form |
Preparer Title |
Phone Number |
Date Form Prepared |
E |
SURROGATE SELECTED BY CONSENSUS OF INTERESTED PERSONS |
(Legally Authorized Representaive as outlined in secion D) |
|
I make this declaraion under the penalty of false swearing to establish my authority to act as the legally authorized represen- |
|
|
taive for the paient named on this form. The paient has been determined by the primary physician to lack decisional |
capacity and no health care agent or court appointed guardian or
|
Signature (required) |
Name |
Relaionship |
|
|
|
|
Compleing POLST
DIRECTIONS FOR HEALTH CARE PROFESSIONAL
•Must be completed by health care professional based on paient preferences and medical indicaions.
•POLST must be signed by a Physician or Advanced Pracice Registered Nurse (APRN) licensed in the state of Hawai‘i and the paient or the paient’s legally authorized representaive to be valid. Verbal orders by providers are not acceptable.
•Use of original form is strongly encouraged. Photocopies and FAXes of signed POLST forms are legal and valid.
Using POLST
• Any incomplete secion of POLST implies full treatment for that secion. Secion A:
• No defibrillator (including automated external defibrillators) should be used on a person who has chosen “Do Not Atempt Resuscitaion.”
Secion B:
•When comfort cannot be achieved in the current seing, the person, including someone with “Comfort Measures Only,” should be transferred to a seing able to provide comfort (e.g., treatment of a hip fracture).
•IV medicaion to enhance comfort may be appropriate for a person who has chosen “Comfort Measures Only.”
•A person who desires IV fluids should indicate “Limited Intervenions” or “Full Treatment.”
Secion C:
• A paient or a legally authorized representaive may make decisions regarding arficial nutriion or hydraion. However, a surrogate who has not been designated by the paient (surrogate selected by consensus of interested persons) may only make a decision to withhold or withdraw arificial nutriion and hydraion when the primary physician and a second independent physician cerify in the paient’s medical records that the provision or coninuaion of arificial nutriion or hydraion is merely prolonging the act of dying and the paient is highly unlikely to have any neurological response in the future. HRS
Reviewing POLST
It is recommended that POLST be reviewed periodically. Review is recommended when:
•The person is transferred from one care seing or care level to another, or
•There is a substanial change in the person’s health status, or
•The person’s treatment preferences change.
Modifying and Voiding POLST
•A person with capacity or, if lacking capacity the legally authorized representaive, can request a different treatment plan and may revoke the POLST at any ime and in any manner that communicates an intenion as to this change.
•To void or modify a POLST form, draw a line through Secions A through E and write “VOID” in large leters on the original and all copies. Sign and date this line. Complete a new POLST form indicaing the modificaions.
•The paient’s provider may medically evaluate the paient and recommend new orders based on the paient’s current health status and goals of care.
Kōkua Mau – Hawai‘i Hospice and Palliaive Care Organizaion
Kōkua Mau is the lead agency for implementaion of POLST in Hawai‘i. Visit www.kokuamau.org/polst to download a copy
or find more POLST informaion. This form has been adopted by the Department of Health July 2014
Kōkua Mau • PO Box 62155 • Honolulu HI 96839 • [email protected] • www.kokuamau.org
SEND FORM WITH PERSON WHENEVER TRANSFERRED OR DISCHARGED
| Fact Name | Description |
|---|---|
| Purpose of POLST | The POLST form is designed to communicate a patient’s preferences for life-sustaining treatment based on their current medical condition. |
| Legal Basis | In Hawaii, the POLST form is governed by Hawai‘i Revised Statutes §327E, which outlines the use and authority of advance directives. |
| Completion Requirements | The form must be signed by a licensed physician or Advanced Practice Registered Nurse (APRN) in Hawaii, along with the patient or their legally authorized representative. |
| Treatment Preferences | Sections of the POLST form allow patients to specify their preferences for resuscitation, medical interventions, and nutrition. |
| HIPAA Compliance | The form complies with HIPAA regulations, allowing healthcare professionals to share POLST information as necessary for patient care. |
| Revocation | Patients or their legally authorized representatives can revoke or modify the POLST at any time, simply by communicating their intention. |
| Periodic Review | It is recommended that the POLST form be reviewed periodically, especially when a patient’s health status changes or they are transferred between care settings. |
| Use of Copies | While the original POLST form is encouraged, photocopies and faxed versions of signed forms are also considered valid and legal. |
Filling out the Hawaii POLST form is a straightforward process that ensures a person's medical preferences are documented and communicated effectively. This form should be completed with care, as it reflects the individual's wishes regarding medical treatment in various situations. Follow these steps to fill out the form correctly.
After filling out the form, it is essential to keep it updated. Changes in health status or treatment preferences should prompt a review of the POLST. This ensures that the medical orders reflect the patient's current wishes and needs.
What is the Hawaii POLST form?
The Hawaii Provider Orders for Life-Sustaining Treatment (POLST) form is a medical document. It outlines a person's preferences for medical treatment in emergency situations. This form is based on the individual’s current medical condition and wishes. It helps ensure that healthcare providers follow the person's desires regarding life-sustaining measures.
Who should complete the POLST form?
A healthcare professional, such as a physician or an Advanced Practice Registered Nurse (APRN), must complete the POLST form. They will base the orders on the patient's medical preferences and conditions. The patient or their legally authorized representative must also sign the form for it to be valid.
What happens if a section of the POLST form is not completed?
If any section of the POLST form is left blank, it implies that the person desires full treatment for that section. This means that healthcare providers will take all necessary measures unless specified otherwise.
Can the POLST form be modified or revoked?
Yes, a person with capacity, or their legally authorized representative, can request changes to the treatment plan at any time. To modify or void the POLST form, simply draw a line through the relevant sections and write "VOID" on the original and all copies. Then, sign and date this change and complete a new POLST form with the desired modifications.
What should be done with the POLST form during transfers?
The POLST form must be sent with the patient whenever they are transferred or discharged from a healthcare facility. This ensures that all healthcare professionals involved in the patient's care are aware of their treatment preferences.
How often should the POLST form be reviewed?
It is recommended to review the POLST form periodically. A review is especially important when the person is transferred to a different care setting, experiences a significant change in health status, or if their treatment preferences change.
What if the patient cannot make decisions about their care?
If a patient lacks decisional capacity, a legally authorized representative can make decisions on their behalf. This representative may be a designated agent, a guardian, or a surrogate chosen by a consensus of interested persons. They must act in the best interest of the patient.
Where can I find more information about the POLST form?
For additional details about the POLST form, you can visit the Kōkua Mau website at www.kokuamau.org/polst. This site provides resources and downloadable copies of the POLST form.
Filling out the Hawaii POLST form is a crucial step in ensuring that a person's healthcare wishes are honored. However, many individuals make mistakes that can lead to confusion or unintended consequences. One common error is failing to complete all sections of the form. Each section is designed to capture specific preferences regarding medical interventions. If a section is left blank, it is interpreted as a desire for full treatment in that area. This can be particularly problematic if the individual has specific wishes that are not clearly expressed.
Another frequent mistake involves misunderstanding the choices regarding cardiopulmonary resuscitation (CPR). Some people may check the "Do Not Attempt Resuscitation" option without fully understanding its implications. This decision should reflect a clear understanding of the individual’s wishes and medical condition. It is essential to discuss this choice with healthcare providers to ensure that it aligns with the person’s values and desires.
Additionally, individuals often overlook the importance of signatures on the POLST form. Both the healthcare provider and the patient or their legally authorized representative must sign the document for it to be valid. Without these signatures, the form may not be honored by healthcare professionals, potentially leading to unwanted treatments or interventions.
Another area of concern is the selection of a surrogate decision-maker. Some individuals might not fully understand the implications of choosing a surrogate selected by consensus of interested persons. This choice can lead to disputes among family members or caregivers about what the individual would have wanted. It’s vital to have clear communication and documentation regarding who is authorized to make decisions on behalf of the person.
Moreover, failing to periodically review the POLST form can result in outdated preferences being followed. As a person's health status changes, so too might their treatment preferences. Regular reviews ensure that the form accurately reflects the individual’s current wishes and medical condition.
Another mistake is neglecting to provide detailed information about the patient's medical condition. The summary section should clearly outline the individual's health status, as this information is crucial for healthcare providers when making treatment decisions. A vague or incomplete summary can lead to misunderstandings about the appropriate level of care.
Lastly, individuals sometimes assume that any healthcare professional can complete the POLST form. However, it must be filled out by a licensed physician or Advanced Practice Registered Nurse (APRN) in Hawaii. Ensuring that the form is completed by the appropriate professional is essential for its validity and effectiveness in guiding treatment decisions.
The Hawaii Physician Orders for Life-Sustaining Treatment (POLST) form is a crucial document for ensuring that a person's healthcare preferences are honored, particularly in emergency situations. However, it often works in conjunction with several other important forms and documents that can provide additional clarity and guidance regarding a person's medical wishes. Below is a list of commonly used documents alongside the POLST form, each serving a unique purpose.
Understanding these documents and their roles can empower individuals to make informed decisions about their healthcare. By utilizing the POLST form alongside these other forms, patients can create a comprehensive plan that reflects their values and preferences, ensuring that their wishes are honored throughout their medical care journey.
The Hawaii POLST (Provider Orders for Life-Sustaining Treatment) form is designed to communicate a patient's preferences regarding medical treatment in emergency situations. Several other documents serve similar purposes in guiding healthcare decisions. Below is a list of seven documents that share similarities with the Hawaii POLST form:
When filling out the Hawaii POLST form, it's important to ensure that the process is done correctly to reflect the patient's wishes and medical needs. Here are nine guidelines to follow:
Following these guidelines can help ensure that the POLST form accurately represents the patient’s wishes and provides clear instructions for their care. It's a crucial step in honoring the dignity and respect that every individual deserves.
There are many misunderstandings surrounding the Hawaii Provider Orders for Life-Sustaining Treatment (POLST) form. Here are six common misconceptions, along with clarifications to help you better understand this important document.
Understanding these misconceptions can help individuals make informed decisions about their healthcare preferences and ensure that their wishes are respected. Always consult with healthcare professionals for guidance on completing and using a POLST form effectively.
Filling out and using the Hawaii POLST form is a crucial step in ensuring that medical care aligns with a person's wishes. Here are some key takeaways to keep in mind:
By keeping these takeaways in mind, individuals and families can better navigate the complexities of medical care preferences in Hawaii.