The Hawaii HC-5 form plays a crucial role in ensuring that employees understand their rights and responsibilities regarding health care coverage under the state’s Prepaid Health Care Act. Designed for individuals who work for multiple employers or are seeking to change their health care status, this form allows employees to notify their principal and secondary employers about their health coverage needs. Whether you are claiming an exemption, terminating an existing waiver, or simply designating which employer will provide your health care, the HC-5 form serves as an essential tool in managing your health care options. It's important to note that this form should only be used under specific circumstances, such as when you work for two or more employers for at least 20 hours a week. By completing this form, you can clarify your health care coverage status, ensuring that your employers are aware of their obligations. Furthermore, it provides a structured way to communicate any changes in your coverage needs, allowing you to navigate the complexities of health care with confidence.
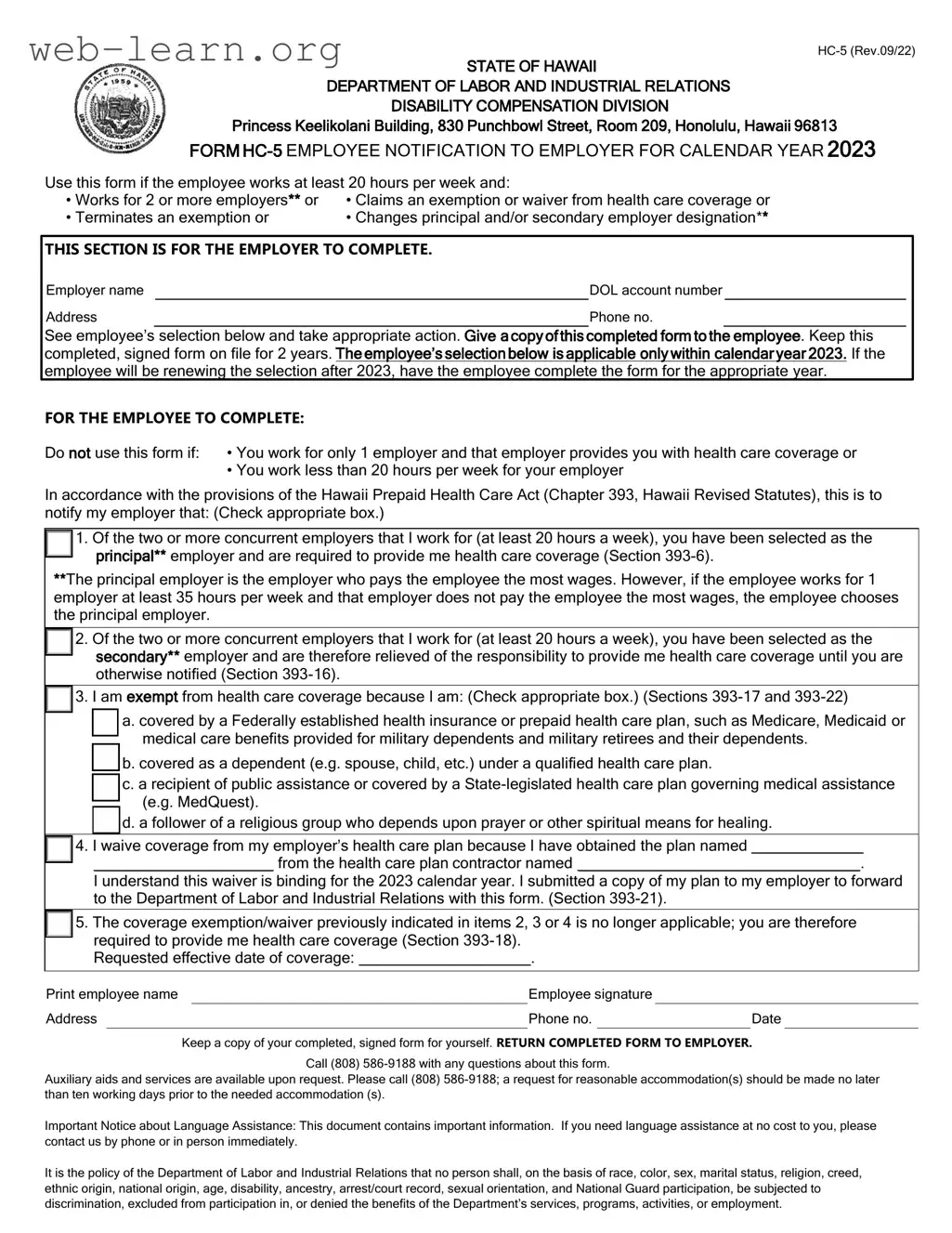
STATE OF HAWAII
DEPARTMENT OF LABOR AND INDUSTRIAL RELATIONS
DISABILITY COMPENSATION DIVISION
Princess Keelikolani Building, 830 Punchbowl Street, Room 209, Honolulu, Hawaii 96813
FORM
Use this form if the employee works at least 20 hours per week and:
•Works for 2 or more employers** or • Claims an exemption or waiver from health care coverage or
• Terminates an exemption or |
• Changes principal and/or secondary employer designation** |
|
|||
|
|
||||
THIS SECTION IS FOR THE EMPLOYER TO COMPLETE. |
|
||||
Employer name |
|
|
DOL account number |
|
|
Address |
|
Phone no. |
|
||
See employee’s selection below and take appropriate action. Give a copy of this completed form to the employee. Keep this completed, signed form on file for 2 years. The employee’s selection below is applicable only within calendar year 2023. If the employee will be renewing the selection after 2023, have the employee complete the form for the appropriate year.
FOR THE EMPLOYEE TO COMPLETE:
Do not use this form if: • You work for only 1 employer and that employer provides you with health care coverage or
•You work less than 20 hours per week for your employer
In accordance with the provisions of the Hawaii Prepaid Health Care Act (Chapter 393, Hawaii Revised Statutes), this is to notify my employer that: (Check appropriate box.)
1. Of the two or more concurrent employers that I work for (at least 20 hours a week), you have been selected as the principal** employer and are required to provide me health care coverage (Section
**The principal employer is the employer who pays the employee the most wages. However, if the employee works for 1 employer at least 35 hours per week and that employer does not pay the employee the most wages, the employee chooses the principal employer.
2. Of the two or more concurrent employers that I work for (at least 20 hours a week), you have been selected as the secondary** employer and are therefore relieved of the responsibility to provide me health care coverage until you are otherwise notified (Section
3. I am exempt from health care coverage because I am: (Check appropriate box.) (Sections
a. covered by a Federally established health insurance or prepaid health care plan, such as Medicare, Medicaid or medical care benefits provided for military dependents and military retirees and their dependents.
b. covered as a dependent (e.g. spouse, child, etc.) under a qualified health care plan.
c. a recipient of public assistance or covered by a
d. a follower of a religious group who depends upon prayer or other spiritual means for healing.
4. I waive coverage from my employer’s health care plan because I have obtained the plan named _____________
_____________________ from the health care plan contractor named _________________________________.
I understand this waiver is binding for the 2023 calendar year. I submitted a copy of my plan to my employer to forward to the Department of Labor and Industrial Relations with this form. (Section
5. The coverage exemption/waiver previously indicated in items 2, 3 or 4 is no longer applicable; you are therefore required to provide me health care coverage (Section
Requested effective date of coverage: ____________________.
Print employee name |
|
|
Employee signature |
|
|
|
||
Address |
|
|
|
Phone no. |
|
|
Date |
|
|
|
Keep a copy of your completed, signed form for yourself. RETURN COMPLETED FORM TO EMPLOYER. |
||||||
Call (808)
Auxiliary aids and services are available upon request. Please call (808)
Important Notice about Language Assistance: This document contains important information. If you need language assistance at no cost to you, please contact us by phone or in person immediately.
It is the policy of the Department of Labor and Industrial Relations that no person shall, on the basis of race, color, sex, marital status, religion, creed, ethnic origin, national origin, age, disability, ancestry, arrest/court record, sexual orientation, and National Guard participation, be subjected to discrimination, excluded from participation in, or denied the benefits of the Department’s services, programs, activities, or employment.
| Fact Name | Fact Description |
|---|---|
| Form Purpose | This form notifies employers of an employee's health care coverage status and any changes in employer designation. |
| Applicable Law | The form is governed by the Hawaii Prepaid Health Care Act, specifically under Chapter 393 of the Hawaii Revised Statutes. |
| When to Use | Employees should use this form if they work for multiple employers, are claiming an exemption, or are changing their employer designation. |
| Employer Responsibilities | Employers must provide health care coverage as indicated in the form and retain a copy for two years. |
| Exemption Criteria | Exemptions can apply if the employee is covered by a federal health plan, a dependent under a qualified plan, or follows a religious group for healing. |
| Submission Guidelines | The form should not be submitted to the State Department of Labor unless requested. It must be renewed annually by December 31. |
Completing the Hawaii HC-5 form is a straightforward process. This form is essential for notifying your employer about your health care coverage status. After filling it out, you will need to keep a copy for your records and submit the completed form to your employer.
Once completed, ensure you keep a copy for your records. Submit the form to your employer, who will retain it for their records. Remember that this form must be renewed every December 31.
What is the Hawaii HC-5 form?
The Hawaii HC-5 form is a notification document that employees use to inform their employers about their health care coverage status under the Hawaii Prepaid Health Care Act. It is specifically designed for employees who work for two or more employers, are claiming an exemption or waiver from health care coverage, or are changing their employer designation.
Who should use the HC-5 form?
This form is intended for employees who:
However, if an employee works for only one employer that provides health care coverage or works less than 20 hours per week, they should not use this form.
What information do I need to complete the HC-5 form?
To fill out the HC-5 form, you will need the following information:
What should I do after completing the HC-5 form?
After you have completed and signed the HC-5 form, keep a copy for your records. You should then provide the completed form to your employer. It is essential that your employer receives this notification to ensure compliance with health care coverage requirements.
How long should my employer keep the HC-5 form?
Your employer is required to keep the completed and signed HC-5 form for a minimum of two years. This retention is important for record-keeping and compliance purposes.
Where can I get assistance if I have questions about the HC-5 form?
If you have any questions regarding the HC-5 form, you can call the Department of Labor and Industrial Relations at (808) 586-9188. They can provide guidance and clarify any concerns you may have about the form or the health care coverage requirements.
Filling out the Hawaii HC-5 form can be straightforward, but many people make common mistakes that can lead to complications. One major error is not keeping a copy of the completed form. It's essential to have a record for your own reference, especially if any questions arise later.
Another frequent mistake is failing to provide accurate employer information. Make sure to double-check the employer's name, address, and DOL account number. Incorrect details can delay the processing of your health care coverage.
Many individuals also overlook the importance of selecting the correct box on the form. Whether you are identifying your principal or secondary employer, or claiming an exemption, it is crucial to check the right option. Misunderstanding your employment situation can lead to incorrect health care coverage assignments.
People often forget to sign and date the form. A signature is necessary to validate your submission. Without it, the form may be considered incomplete, causing further delays in your coverage.
Another common issue is not understanding the requirements for exemptions. For example, if you claim an exemption based on coverage from another plan, ensure that you provide the name of that plan and its contractor. Failing to do so can result in the denial of your exemption.
Some individuals mistakenly believe they can use this form even if they work for only one employer that provides health care coverage. This form is only for those with multiple employers or specific exemption needs. Using it incorrectly can lead to unnecessary confusion.
Additionally, people sometimes ignore the requirement to inform their employer if their exemption or waiver status changes. If you no longer meet the criteria for exemption, you must notify your employer promptly. Not doing so can result in a lapse in coverage.
Finally, many forget about the renewal requirement. The form must be renewed every December 31. If you don’t submit a new form, your coverage might be affected, leading to gaps in health care benefits.
The Hawaii HC-5 form serves as an important notification tool for employees regarding their health care coverage responsibilities under the Hawaii Prepaid Health Care Act. Several other forms and documents are commonly utilized in conjunction with the HC-5 to ensure compliance and clarity regarding health care coverage and employment status. Below is a list of these forms, each described briefly to provide a better understanding of their purpose.
Understanding these associated forms can facilitate a smoother process for both employees and employers in navigating health care coverage requirements in Hawaii. Proper completion and submission of these documents help maintain compliance with state regulations and protect the rights of employees regarding their health care benefits.
The Hawaii HC 5 form serves specific purposes related to employee health care coverage under the Hawaii Prepaid Health Care Act. Here are eight documents that are similar to the HC 5 form, along with their key similarities:
When filling out the Hawaii HC-5 form, it’s crucial to follow specific guidelines to ensure your submission is accurate and effective. Here’s a list of important do’s and don’ts to keep in mind:
By adhering to these guidelines, you can help ensure that your health care coverage needs are met without unnecessary complications. Take action now to avoid any delays in your coverage!
The Hawaii HC 5 form is an important document for employees working in multiple jobs or those seeking health care coverage exemptions. However, there are several misconceptions surrounding this form that can lead to confusion. Below is a list of common misconceptions along with explanations to clarify each point.
This form is also applicable for individuals who are seeking an exemption or waiver from health care coverage, regardless of how many employers they have.
It is essential for employees to retain a copy of the completed and signed HC 5 form for their records. This can help in future discussions with employers regarding health care coverage.
Employees should not submit this form to the State Department of Labor unless specifically requested. Instead, it should be given to the employer and kept for personal records.
The form needs to be renewed every December 31, but not all employees will need to fill it out each year. It depends on changes in employment status or health care coverage.
While the form notifies employers of an employee's health care needs, it does not guarantee coverage. Employers must comply based on the information provided in the form.
Employees must designate the employer who pays the most wages as their principal employer, unless they work at least 35 hours a week for another employer who does not pay the most wages.
Employees who waive coverage through the HC 5 form can still receive health care benefits from other plans that meet the requirements of the Prepaid Health Care Act.
This form is relevant for employees who work at least 20 hours per week, regardless of whether they are full-time or part-time across multiple jobs.
Employees receiving public assistance may still need to complete the HC 5 form if they are working and wish to notify their employers about their health care coverage status.
Filling out the Hawaii HC-5 form is an important step for employees who need to communicate their health care coverage status to their employers. Here are some key takeaways to keep in mind:
By following these guidelines, you can ensure that your health care coverage is properly managed and that your rights are upheld.