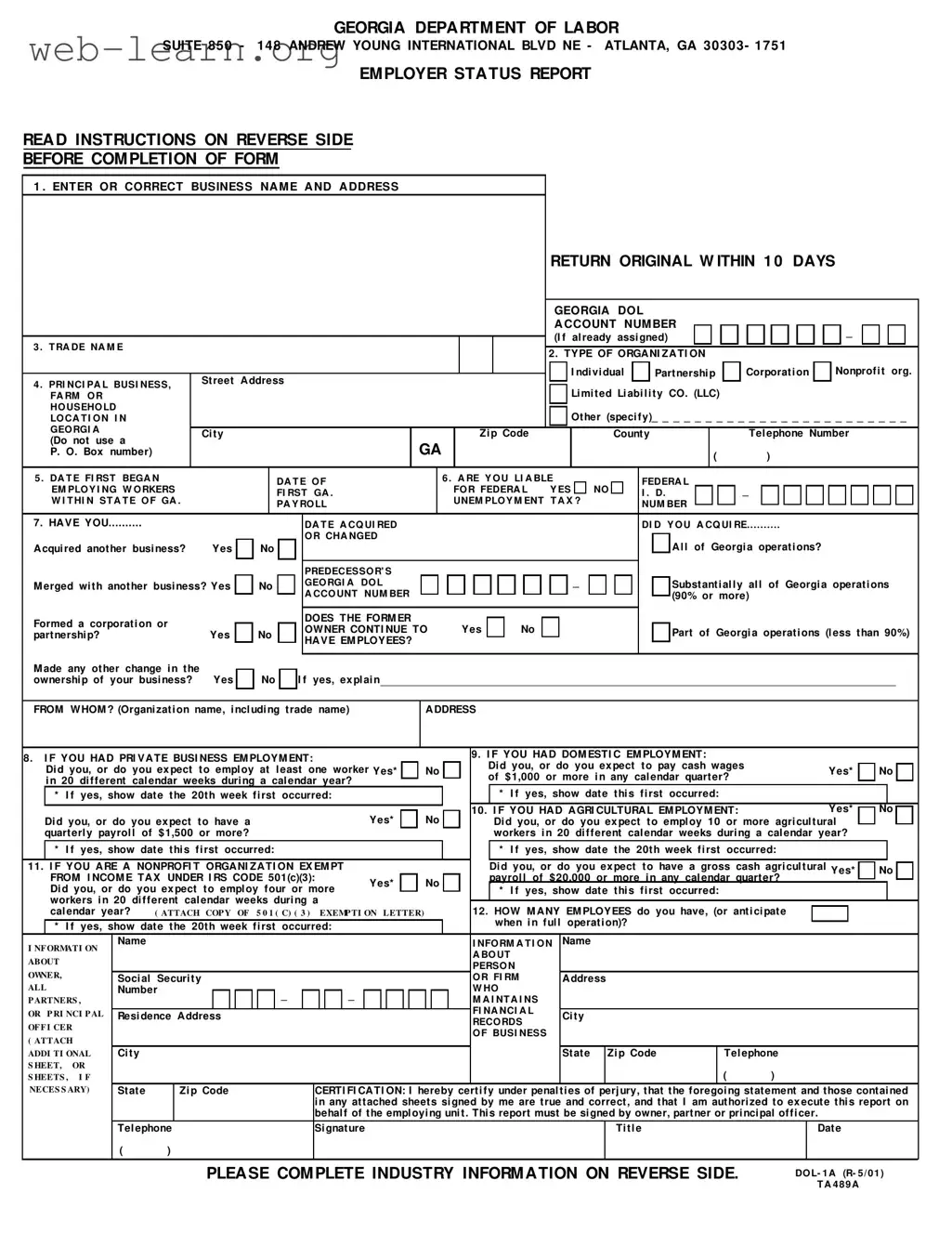
The Georgia Department of Labor form, commonly known as the Employer Status Report, plays a crucial role for businesses operating within the state. This form requires employers to provide essential information about their business, including the name and address, type of organization, and the nature of their operations. It also prompts employers to disclose their Georgia Department of Labor account number if one has been assigned. The form asks specific questions regarding employment status, such as whether the business has employees, the type of employment (private, domestic, or agricultural), and any changes in ownership or business structure. Employers must also report their anticipated number of employees and the gross payroll amounts expected for various types of employment. Additionally, nonprofit organizations must confirm their tax-exempt status under IRS Code 501(c)(3) and provide supporting documentation. Completing this form accurately and submitting it within ten days is not just a regulatory requirement; it is vital for ensuring compliance with state employment laws and maintaining good standing with the Georgia Department of Labor.
| Fact Name | Details |
|---|---|
| Purpose | The Georgia Employer Status Report is designed to collect information about employers operating in Georgia. |
| Filing Deadline | Employers must return the original form within 10 days of completion. |
| Types of Organizations | Organizations can be classified as Individual, Partnership, Corporation, Nonprofit, or Limited Liability Company (LLC). |
| Governing Law | This form is governed by the Employment Security Law, specifically OCGA Section 34-8-121. |
| Federal Tax Identification | Employers must provide their Federal Employer Identification Number if applicable, regardless of their liability status. |
| Nonprofit Requirements | Nonprofit organizations must attach a copy of their IRS exemption letter under Section 501(c)(3) if applicable. |
| Criminal Penalties | Providing false information or failing to submit the report can lead to criminal charges, with each day of non-compliance considered a separate offense. |
Completing the Georgia Department of Labor form is an important step for employers in the state. It is essential to provide accurate information to ensure compliance with state regulations. Below are the steps to guide you through filling out the form effectively.
Once the form is filled out, it must be returned to the Georgia Department of Labor within ten days. Ensure that all information is accurate to avoid any potential issues. Retaining a copy for your records is also advisable.
What is the purpose of the Georgia Department of Labor form?
The Georgia Department of Labor form, specifically the Employer Status Report, is designed to collect essential information from employers operating in Georgia. It ensures that the Department has accurate records of businesses that employ individuals in the state, which is crucial for tax and employment regulations.
Who needs to complete this form?
All employers who have individuals performing services in Georgia must complete this form. This requirement applies regardless of the number of employees or the duration of their employment. The form must be filed when a business first employs workers in Georgia or when there is a change in ownership or structure.
What information is required on the form?
The form requests various details, including:
Completing all sections accurately is essential for compliance.
What happens if the form is not filed on time?
Failure to file the Employer Status Report within the required ten days can lead to penalties. Each day of non-compliance may be considered a separate offense, and this can result in fines or other legal consequences.
How can I submit the completed form?
The completed form must be returned to the Georgia Department of Labor within ten days of completion. Employers should mail the original form to the specified address provided on the form. It is advisable to retain a copy for personal records.
What if my business is a nonprofit organization?
Nonprofit organizations must indicate their status on the form and attach a copy of their IRS exemption letter under Section 501(c)(3). This documentation is essential to validate their tax-exempt status and ensure compliance with state regulations.
Are there specific employment thresholds I should be aware of?
Yes, the form includes questions regarding employment thresholds. For example, if you expect to employ at least one worker in 20 different calendar weeks during a calendar year, or if you anticipate cash wages of $1,000 or more in any calendar quarter, these must be indicated on the form.
What should I do if I have multiple business locations in Georgia?
If your business operates in multiple locations within Georgia, you must provide information for each location on the form. This includes the nature of business and the percentage of income derived from each location. Additional sheets can be attached if necessary.
How can I get assistance if I have questions about the form?
If you require assistance, you can contact the Georgia Department of Labor's Adjudication Section at (404) 232-3301 or the Industry Classification Unit at (800) 338-2082. They can provide guidance on completing the form and addressing any specific inquiries you may have.
Completing the Georgia Department of Labor form can be straightforward, but several common mistakes can lead to delays or complications. One frequent error occurs when individuals fail to provide the correct business name and address. It is crucial to enter or correct this information accurately, as it determines where correspondence and reports will be sent. Missing or incorrect details can result in the need for resubmission, wasting valuable time.
Another common mistake is neglecting to indicate the type of organization. The form requires a check mark next to the appropriate category, such as Individual, Partnership, Corporation, or Nonprofit. Failing to do this can lead to confusion regarding the business's legal structure and may affect tax liabilities and compliance obligations.
Additionally, many individuals overlook the necessity of providing the Georgia Department of Labor Account Number if one has already been assigned. This number is essential for tracking the business’s employment status and history. Not including it can complicate the processing of the form and may lead to unnecessary follow-up actions.
Lastly, individuals often forget to sign the form. Certification is a critical step, as it confirms the accuracy of the information provided. Without a signature from the owner, partner, or principal officer, the form cannot be processed. This oversight can lead to delays and may require the form to be resubmitted, further complicating the reporting process.
The Georgia Department of Labor form is a crucial document for employers operating within the state. It serves as an Employer Status Report, capturing essential information about a business's employment status and obligations. Alongside this form, several other documents are often required or beneficial for compliance with labor regulations. Below is a list of related forms and documents commonly used in conjunction with the Georgia Department of Labor form.
Understanding these documents and their purposes is vital for compliance with state and federal labor laws. Employers should ensure that they are accurately completing and submitting these forms to avoid potential legal issues and to maintain good standing with regulatory agencies.
The Georgia Department of Labor form serves a specific purpose in reporting employer status, but it shares similarities with several other important documents that businesses may encounter. Here’s a look at eight such documents:
Understanding these documents and their similarities can help ensure compliance and streamline the administrative processes involved in running a business.
When filling out the Georgia Department of Labor form, it is important to follow certain guidelines to ensure accuracy and compliance. Here is a list of things you should and shouldn't do:
Misconceptions about the Georgia Department of Labor form can lead to confusion and delays in compliance. Here are eight common misconceptions explained:
Understanding these misconceptions can help ensure compliance with Georgia's labor laws and avoid unnecessary complications.
Key Takeaways for Filling Out the Georgia Department of Labor Form: