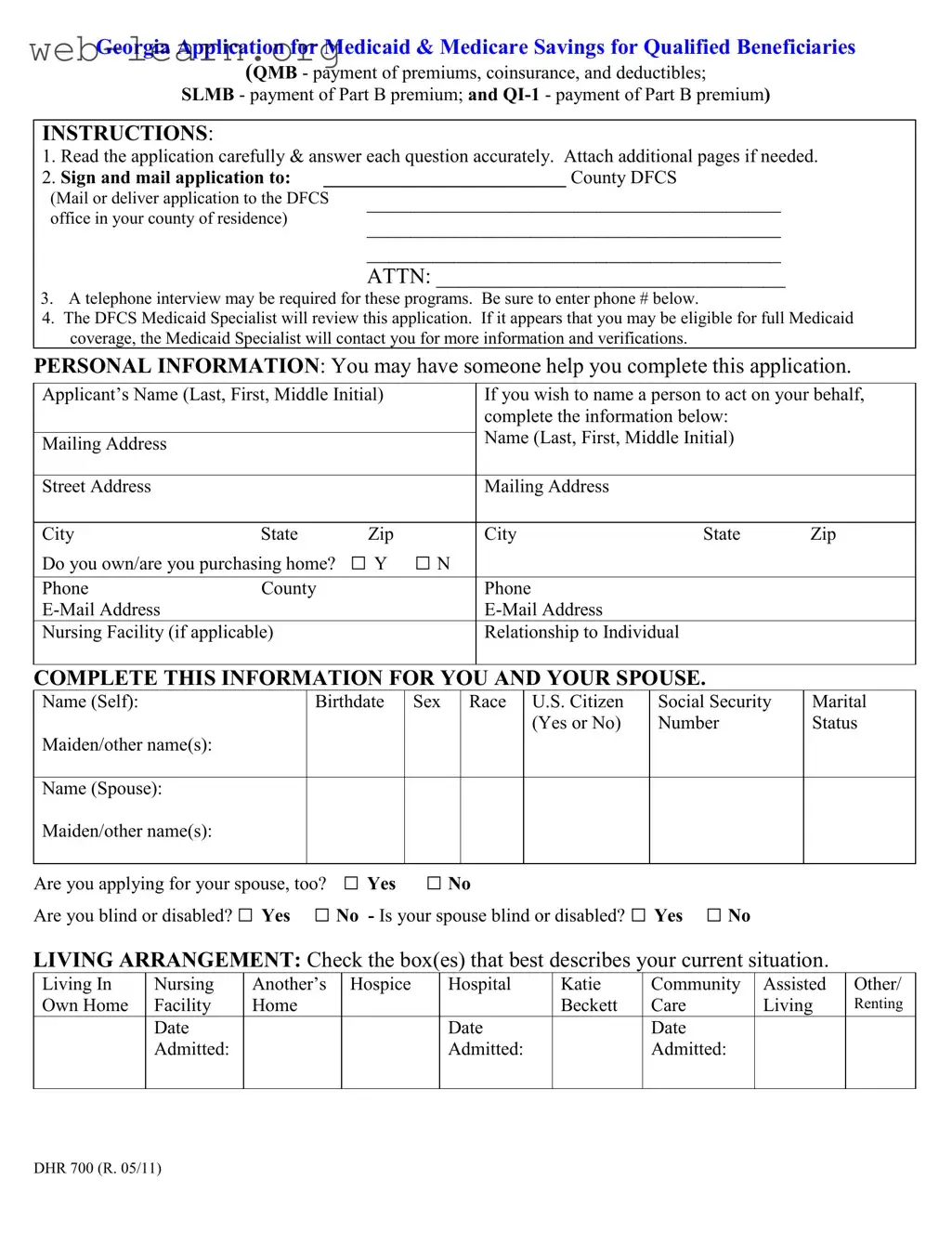
The Georgia Application for Medicaid is a crucial document for individuals seeking assistance with healthcare costs. This form serves multiple purposes, including applying for Medicaid and Medicare Savings for Qualified Beneficiaries. It encompasses various programs such as the Qualified Medicare Beneficiary (QMB), which covers premiums, coinsurance, and deductibles; the Specified Low-Income Medicare Beneficiary (SLMB), which assists with Part B premiums; and the Qualified Individual (QI-1) program, also aimed at covering Part B premiums. Completing the application requires careful attention to detail, as applicants must provide personal information, including names, addresses, and Social Security numbers. The form also requests details about living arrangements, health insurance coverage, assets, income, and resources. Additionally, applicants may need to include information about their spouse and any other individuals they are applying for. A signature is required to confirm the accuracy of the information provided, and applicants should be prepared for a possible telephone interview. Understanding these components is essential for a smooth application process and to ensure that all necessary information is accurately reported.
| Fact Name | Details |
|---|---|
| Form Title | Georgia Application for Medicaid & Medicare Savings for Qualified Beneficiaries |
| Governing Laws | Georgia Medicaid Program regulations and federal Medicaid laws |
| Purpose | This form is used to apply for Medicaid and Medicare savings programs for eligible individuals. |
| Eligibility Programs | Includes Qualified Medicare Beneficiary (QMB), Specified Low-Income Medicare Beneficiary (SLMB), and Qualifying Individual (QI-1). |
| Submission Method | Applicants must mail or deliver the completed application to their local County DFCS office. |
| Interview Requirement | A telephone interview may be required for applicants seeking these benefits. |
| Personal Assistance | Applicants may have someone assist them in completing the application. |
| Privacy Statement | Confidential information is protected by federal and state laws concerning applicants and recipients. |
| Signature Requirement | Applicants must sign the form to certify the accuracy of the information provided. |
| Estate Recovery Program | Medicaid members may be subject to recovery of medical assistance payments from their estate after death. |
Filling out the Georgia Application for Medicaid can be a straightforward process if you follow the steps carefully. After completing the form, it will need to be submitted to your county's Department of Family and Children Services (DFCS) office. A review will follow, and you may be contacted for further information if necessary.
What is the Georgia Application for Medicaid?
The Georgia Application for Medicaid is a form that individuals must complete to apply for Medicaid benefits in the state of Georgia. This application helps determine eligibility for various programs, including Medicaid and Medicare Savings for Qualified Beneficiaries, which can assist with costs related to healthcare premiums, coinsurance, and deductibles.
Who can help me fill out the application?
You are allowed to have someone assist you in completing the application. This could be a family member, friend, or a professional who understands the requirements. It is important that the information provided is accurate and complete, as this will affect your eligibility for benefits.
What personal information do I need to provide?
The application requires various personal details, including:
Make sure to provide accurate and complete information to avoid delays in processing your application.
What happens after I submit the application?
Once your application is submitted, a Medicaid Specialist from the Division of Family and Children Services (DFCS) will review it. If the specialist believes you may qualify for full Medicaid coverage, they will reach out for additional information or verification. Be prepared for a possible telephone interview as part of this process.
What types of income should I report?
It is crucial to list all sources of income accurately. This includes:
Reporting your income correctly helps ensure that you receive the benefits you may be entitled to.
What if I have other health insurance?
If you or your spouse has other health insurance, you must disclose this information on the application. The form will ask for details about your coverage, including the type of insurance and the effective dates. This information is necessary for determining how Medicaid may coordinate with your existing coverage.
Are there any assets I need to disclose?
Yes, the application requires you to report all assets, including real estate, vehicles, bank accounts, and any other resources. This includes assets owned jointly with others. Be thorough in this section, as failing to disclose assets can affect your eligibility.
What is the privacy statement about?
The privacy statement included in the application assures you that your personal information will be kept confidential and used only for purposes directly related to the administration of Medicaid programs. It is important to understand that your information may be verified with other agencies to confirm eligibility.
What should I do if I disagree with a decision made on my application?
If you disagree with any decision made by the agency regarding your application, you have the right to request a fair hearing. This allows you to present your case and seek a resolution. You may also choose to have someone represent you during this process.
Filling out the Georgia Application for Medicaid can be a complex process, and many applicants make common mistakes that can delay their eligibility or even lead to denials. One frequent error is failing to read the application instructions thoroughly. The application clearly states the importance of answering each question accurately. Skipping questions or providing incomplete information can result in the application being returned or delayed. It is crucial to take the time to understand what is being asked and ensure that all sections are filled out completely.
Another common mistake involves not providing sufficient documentation. The application requires supporting documents, such as proof of income, resources, and health insurance. Applicants often overlook this requirement, thinking that their answers alone will suffice. It is essential to attach copies of necessary documents, like Medicare and insurance cards, as specified in the instructions. Without this documentation, the application may be considered incomplete, leading to further complications.
Many applicants also underestimate the significance of accuracy in reporting income and resources. It is vital to list all types of income before any deductions, including Social Security, wages, and any other benefits received. Some people mistakenly report net income instead of gross income, which can misrepresent their financial situation. Additionally, failing to disclose all resources, such as bank accounts or property, can lead to serious consequences, including potential legal issues.
Another mistake is neglecting to include contact information for follow-up. The application mentions that a telephone interview may be required. Providing an incorrect or missing phone number can hinder communication with the Medicaid Specialist, causing delays in the review process. It is advisable to double-check that all contact information is accurate and up to date.
Lastly, applicants often forget to sign and date the application before submitting it. This step is crucial, as the application cannot be processed without a signature. Some individuals may also overlook the importance of the declaration of citizenship or immigration status, which is a critical part of the application. Ensuring that all required signatures are present is necessary to avoid unnecessary delays.
The Georgia Application for Medicaid form is a crucial document for individuals seeking Medicaid benefits. Alongside this application, several other forms and documents are often required to ensure a complete submission and to facilitate the eligibility determination process. Below is a list of commonly used documents that may accompany the Medicaid application.
Submitting these additional documents along with the Georgia Application for Medicaid can streamline the application process and support a thorough review by the Medicaid Specialist. Ensuring all required information is included will help in achieving timely eligibility determinations.
When filling out the Georgia Application for Medicaid form, it is important to follow certain guidelines to ensure the process goes smoothly. Below is a list of things you should and shouldn't do.
Following these guidelines can help facilitate the application process and improve your chances of a successful outcome.
This is not entirely true. While income is a significant factor, eligibility for Medicaid in Georgia also considers other aspects such as assets, age, and disability status.
In fact, you can have someone assist you with the application process. This could be a family member, friend, or advocate who understands the requirements.
While having a Social Security Number is beneficial, there are provisions for individuals who do not have one. It’s important to discuss your situation with the Medicaid office.
Many applicants find that the process can take time. It often involves gathering documentation and potentially undergoing a phone interview, which can extend the timeline.
This is incorrect. You can reapply if your circumstances change or if you believe the denial was in error. Always review the reasons for denial to address any issues.
Not all assets are counted against you. Certain resources, like your primary home and some personal items, may not affect your eligibility.
This is a common misunderstanding. Many individuals qualify for both Medicare and Medicaid, especially if they meet specific criteria regarding income and assets.
You can submit your application by mail or deliver it to your local DFCS office. This flexibility can make the process easier for many applicants.
Approval is not guaranteed. The Medicaid Specialist will review your entire application and may request additional information before making a determination.
Benefits can vary based on individual circumstances, including income, health needs, and the specific Medicaid program for which you qualify. It’s essential to understand what is available to you.