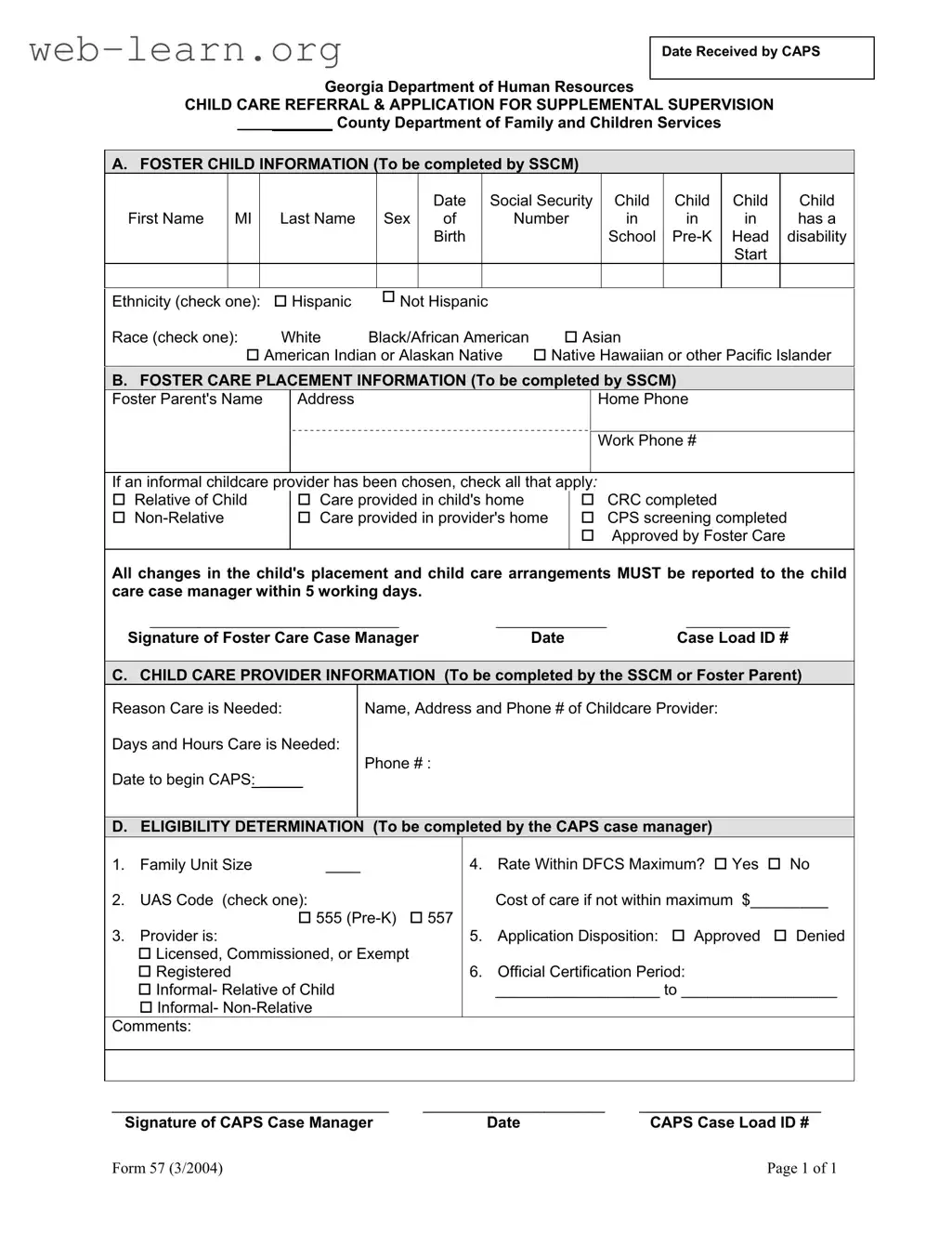
The Georgia 57 form plays a crucial role in the state's child welfare system, specifically concerning foster care and childcare arrangements. This form is primarily used by the Department of Human Resources to facilitate the referral and application process for supplemental supervision of children in foster care. It captures essential information about the foster child, including their name, date of birth, and social security number, as well as details about their disability status and ethnicity. Additionally, the form requires information about the foster care placement, including the foster parent's contact details and the nature of the childcare arrangement, whether with relatives or non-relatives. It also outlines the necessity for timely reporting of any changes in the child's placement or childcare to the case manager. The form further includes sections for determining eligibility, where the case manager assesses family unit size, childcare costs, and whether the provider meets the required standards. Ultimately, the Georgia 57 form is a vital tool for ensuring that children in foster care receive appropriate and timely childcare services while maintaining compliance with state regulations.
| Fact Name | Details |
|---|---|
| Form Title | Child Care Referral & Application for Supplemental Supervision |
| Governing Law | Georgia Department of Human Services regulations |
| Date of Last Update | March 2004 |
| Purpose | This form is used to apply for supplemental supervision for foster children. |
| Required Information | Foster child information, foster care placement details, and child care provider information must be provided. |
| Eligibility Determination | The CAPS case manager assesses eligibility based on family size and care costs. |
| Signature Requirement | Signatures of both the Foster Care Case Manager and CAPS Case Manager are required. |
| Reporting Changes | Any changes in the child's placement or care arrangements must be reported within 5 working days. |
| Confidentiality | All information provided in this form is confidential and used for case management purposes only. |
Completing the Georgia 57 form is a crucial step in ensuring that foster children receive the necessary care and supervision. This form gathers essential information about the child, their foster care placement, and the childcare provider. Following these steps will help you fill out the form accurately and efficiently.
Once the form is filled out, ensure that all required signatures are obtained and that any necessary documentation is attached. Timely submission of the completed form is essential for processing and to avoid delays in care for the child.
What is the purpose of the Georgia 57 form?
The Georgia 57 form is used to apply for supplemental supervision for foster children. It serves as a referral and application document that helps the Department of Family and Children Services assess the need for additional childcare resources for children in foster care.
Who needs to complete the Georgia 57 form?
The form must be completed by the Social Services Case Manager (SSCM) for the foster child. In some sections, the foster parent may also provide necessary information, particularly regarding childcare providers and the reasons for care.
What information is required about the foster child?
Section A of the form collects vital details about the foster child, including:
What details are needed regarding the foster care placement?
In Section B, the form requires information about the foster parent, including:
It is important to report any changes in the child's placement or childcare arrangements within five working days to ensure proper care.
How is the eligibility for childcare determined?
Section D is where the CAPS case manager assesses eligibility. This includes evaluating:
What should I do if my application is denied?
If your application is denied, you may want to review the reasons for denial provided by the CAPS case manager. Understanding these reasons can help you address any issues or gather additional information needed for a potential reapplication.
What is the significance of the signature on the form?
The signatures of both the foster care case manager and the CAPS case manager validate the information provided and confirm that the application has been reviewed. This step is crucial for the processing of the application.
How often should I update the information on the Georgia 57 form?
Any changes in the child’s placement or childcare arrangements should be reported within five working days. Regular updates ensure that the child receives the appropriate level of care and support.
Filling out the Georgia 57 form can be a straightforward process, but several common mistakes can lead to delays or issues in approval. One of the most frequent errors occurs in the section regarding foster child information. Many applicants fail to provide complete information, such as the child’s full name, date of birth, or Social Security number. Omitting any of these details can result in processing delays. Ensure that all fields are filled out accurately and completely to avoid unnecessary complications.
Another common mistake involves the foster care placement information. Applicants often overlook the requirement to report any changes in the child’s placement or childcare arrangements within five working days. This oversight can lead to compliance issues and may affect the child’s eligibility for services. It is essential to stay updated and communicate any changes promptly to the child care case manager.
In the child care provider section, applicants sometimes neglect to provide complete contact information for the childcare provider. This includes the provider’s name, address, and phone number. Incomplete information can hinder the verification process and delay the approval of the application. Always double-check that all necessary details are included before submitting the form.
Finally, applicants may misinterpret the eligibility determination section. Errors in family unit size or UAS code can lead to incorrect assessments of the application. Understanding the definitions and requirements for these fields is crucial. Take the time to review the eligibility criteria and ensure that all selections accurately reflect your situation. Doing so can help facilitate a smoother application process.
The Georgia 57 form is a critical document used in the child care referral and application process for supplemental supervision within the state. This form is often accompanied by several other documents to ensure a comprehensive evaluation of a child's needs and the suitability of their care arrangements. Below are some of the key forms and documents that are frequently utilized alongside the Georgia 57 form.
Understanding these accompanying forms and documents is essential for ensuring that the child’s needs are met effectively. Each document plays a unique role in the overall process, contributing to the welfare and safety of the child in foster care.
The Georgia 57 form is an important document used in the context of child care referrals and applications for supplemental supervision. It serves a specific purpose but shares similarities with several other forms. Here’s a look at five documents that are comparable to the Georgia 57 form, highlighting how they are alike:
When filling out the Georgia 57 form, it's essential to follow specific guidelines to ensure that the application process runs smoothly. Below are some important dos and don'ts to keep in mind.
By following these guidelines, you can help ensure that the Georgia 57 form is completed correctly, making the process easier for everyone involved.
Understanding the Georgia 57 form can be challenging. Here are six common misconceptions that people often have:
Clearing up these misconceptions can help ensure that foster families navigate the process more smoothly and access the support they need.
When filling out and using the Georgia 57 form, there are several important points to keep in mind: