The GED Illinois form serves as a crucial tool for individuals who have completed their GED testing in Cook County, Illinois, allowing them to officially request their GED certificate or transcript of test results. It provides clear instructions for applicants, ensuring they understand the process of obtaining their documents. Eligible individuals may receive these certificates or transcripts at no cost, but specific guidelines must be followed to avoid unnecessary fees. The form requires personal information, including the name used during testing, current address, and social security number. Applicants must specify the items they are requesting, along with the applicable fees—$3.00 for each transcript and $10.00 for each certificate. Additionally, the form outlines the necessary documentation for those who need to update their personal information, such as name changes or corrections to social security numbers. Understanding these details is essential for a smooth application process, and proper completion of the form is vital for timely delivery of requested documents.
| Fact Name | Details |
|---|---|
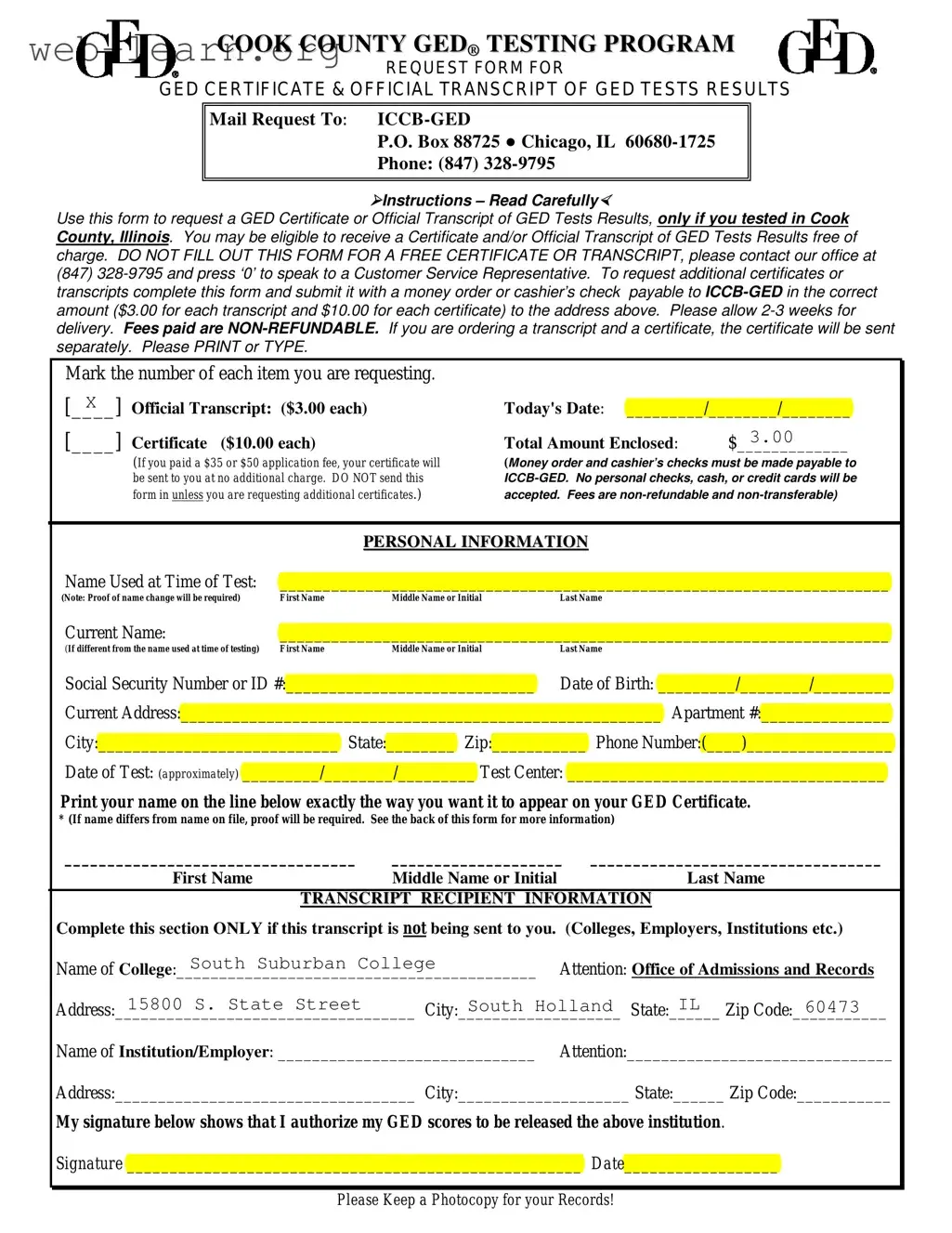
| Purpose | This form is used to request a GED Certificate or Official Transcript of GED Tests Results for individuals who tested in Cook County, Illinois. |
| Eligibility | Individuals may receive a Certificate and/or Official Transcript free of charge under certain conditions. |
| Fees | There is a fee of $3.00 for each transcript and $10.00 for each certificate requested. |
| Payment Method | Payments must be made via money order or cashier’s check payable to ICCB-GED. Personal checks, cash, or credit cards are not accepted. |
| Delivery Time | Requests typically take 2-3 weeks for delivery after submission. |
| Personal Information Required | The form requires the name used at the time of testing, current name, Social Security Number or ID, date of birth, and current address. |
| Governing Laws | This form is governed by the Illinois Community College Board regulations regarding GED testing and certification. |
Filling out the GED Illinois form is a straightforward process. Ensure that you have all the necessary information and documents ready before you begin. This will help you complete the form accurately and efficiently.
What is the purpose of the GED Illinois form?
The GED Illinois form is used to request a GED Certificate or an Official Transcript of GED Test Results for individuals who tested in Cook County, Illinois. This form is essential for obtaining proof of completion of the GED program, which can be required for employment, further education, or personal records.
Who is eligible to use this form?
Only individuals who took the GED tests in Cook County, Illinois, can use this form. If you are unsure about your eligibility or if you are seeking a free certificate or transcript, you should contact the office at (847) 328-9795 for assistance.
What are the fees associated with the GED Illinois form?
There are specific fees for obtaining certificates and transcripts. The cost is $3.00 for each transcript and $10.00 for each certificate. Payments must be made via money order or cashier's check made payable to ICCB-GED. Personal checks, cash, or credit cards are not accepted. All fees are non-refundable.
How long does it take to receive the requested documents?
Once the form and payment are submitted, you should allow 2-3 weeks for delivery of your GED Certificate or Official Transcript. If you are requesting both a certificate and a transcript, they will be sent separately.
What should I do if my name has changed since taking the GED tests?
If your name has changed, you must provide proof of the name change along with your request. Acceptable documents include a photocopy of a marriage license, divorce decree, or court order, as well as a valid form of identification such as a state ID, driver’s license, or passport.
How can I correct my Social Security Number or Date of Birth on my GED records?
To correct your Social Security Number, submit a notarized letter explaining the change, along with a printout from the Social Security Administration and a photocopy of your new Social Security Card. For Date of Birth corrections, provide a photocopy of your birth certificate and a valid form of ID. Ensure all documents are included with your request.
Where should I send my completed GED Illinois form?
Mail your completed form, along with the payment, to the following address:
For any further questions, you can contact the Cook County GED office at (847) 328-9795.
Filling out the GED Illinois form can be a straightforward process, but many individuals make common mistakes that can delay their request for a certificate or transcript. One frequent error involves not providing the correct name used at the time of testing. If a person has changed their name since taking the GED tests, they must ensure that the name they write on the form matches exactly with the records held by the testing authority. Failure to do so may result in complications or even rejection of the application.
Another common mistake is neglecting to include the appropriate payment for the requested documents. The form specifies that each transcript costs $3.00 and each certificate costs $10.00. Applicants often forget to calculate the total amount correctly or fail to include a money order or cashier's check made out to ICCB-GED. Personal checks, cash, or credit cards are not accepted, which can lead to unnecessary delays if the payment method is incorrect.
Some individuals also overlook the requirement to provide proof of name changes when applicable. If the name on the form differs from the name in the GED records, the applicant must submit documentation such as a marriage license, divorce decree, or court order. Without this proof, the request may be stalled until the necessary documents are provided.
Additionally, a common oversight is not filling out the personal information section completely. This section requires details like the Social Security Number, date of birth, and current address. Incomplete or inaccurate information can lead to processing issues, causing further delays in receiving the requested documents.
Finally, some applicants fail to keep a photocopy of their submission. It is crucial to retain a copy of the completed form for personal records. This practice can be beneficial if there are any questions or issues with the request in the future. By avoiding these mistakes, individuals can streamline their experience and ensure a smoother process in obtaining their GED certificates or transcripts.
The GED Illinois form is an essential document for individuals seeking to obtain their GED Certificate or Official Transcript of GED Test Results in Cook County. However, several other forms and documents may accompany the GED Illinois form, each serving a specific purpose in the process. Below is a list of these documents, along with brief descriptions of their functions.
Understanding these documents can streamline the process of obtaining a GED and ensure that all necessary information is accurately submitted. Each form plays a crucial role in maintaining the integrity and accuracy of GED records, ultimately aiding individuals in their educational and professional pursuits.
The GED Illinois form shares similarities with several other documents used for educational and certification purposes. Here are six documents that are similar:
When filling out the GED Illinois form, there are important guidelines to follow. Here’s a list of things you should and shouldn’t do:
Following these guidelines will help ensure a smooth process in obtaining your GED certificate or transcript.
Here are 10 common misconceptions about the GED Illinois form, along with clarifications to help you better understand the process.
Understanding these misconceptions can help streamline your experience when requesting your GED certificate or transcript. If you have further questions, reach out to the Cook County GED office for assistance.
When filling out the GED Illinois form, it is essential to follow specific guidelines to ensure a smooth process. Here are six key takeaways:
By adhering to these guidelines, you can effectively navigate the GED Illinois form process and obtain the necessary documentation.