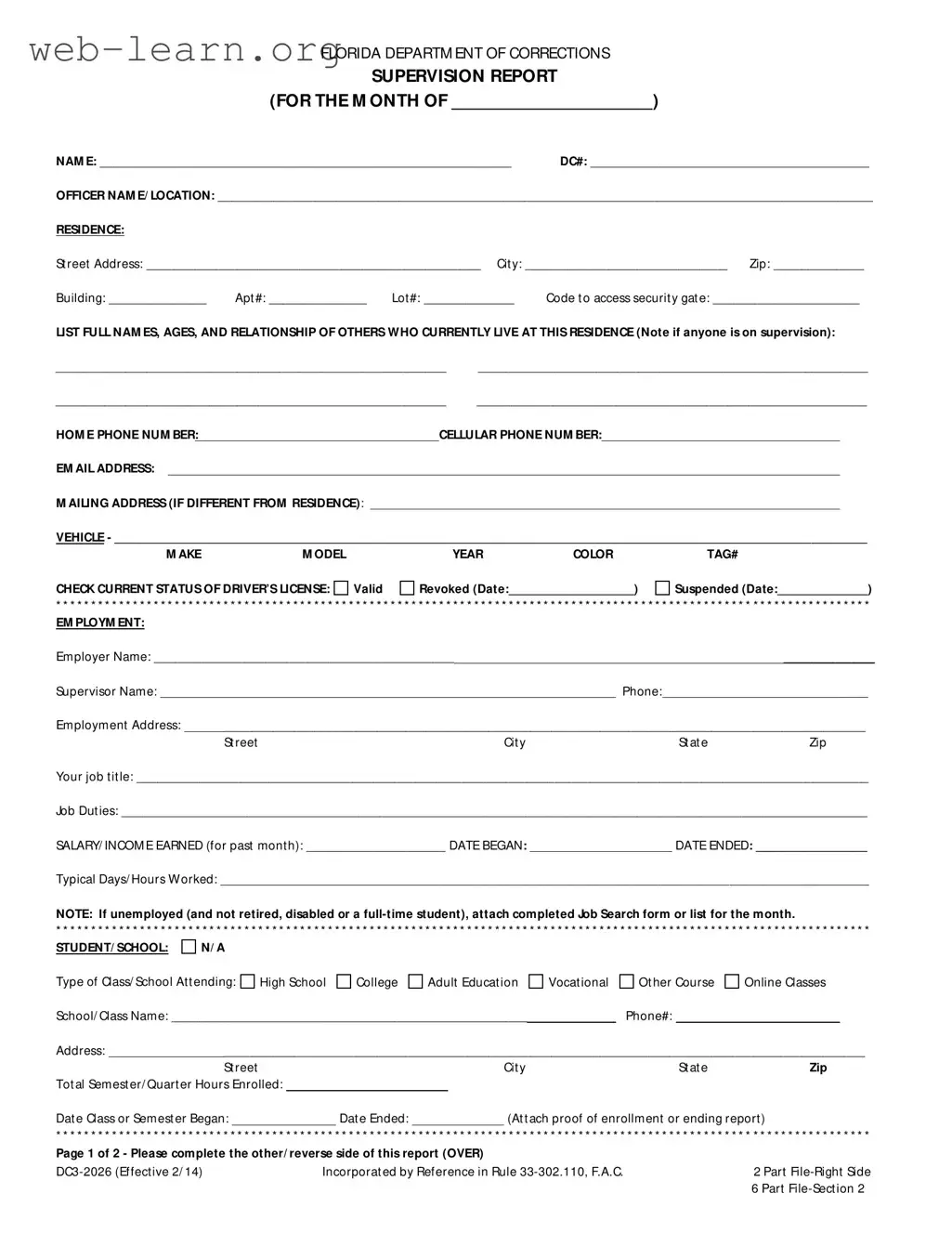
The Florida Supervision Report form serves as a crucial tool for individuals under supervision, providing a structured way to document their progress and compliance with the terms of their supervision. Each month, individuals fill out this form to report on various aspects of their lives, including their residence, employment status, and any educational pursuits. The form requires personal information such as names and relationships of household members, which helps probation officers understand the individual's living situation. Additionally, it includes sections for reporting on special conditions of supervision, such as community service hours and treatment attendance. This ensures that individuals remain accountable for their commitments. Contact with law enforcement, personal goals, and action steps taken towards those goals are also documented, allowing for a comprehensive overview of the individual’s progress. By completing this form, individuals not only fulfill their reporting requirements but also reflect on their achievements and areas for improvement, fostering personal growth and accountability.
| Fact Name | Details |
|---|---|
| Purpose | The Florida Supervision Report is used to track the progress of individuals on probation or supervision. |
| Governing Law | This form is incorporated by reference in Rule 33-302.110 of the Florida Administrative Code. |
| Monthly Requirement | Supervisees must submit this report monthly to their probation officer. |
| Personal Information | The form requires personal details, including name, address, and contact information. |
| Employment Details | Supervisees must provide information about their employment status and job duties. |
| Education Status | Educational information is also required, including school name and enrollment dates. |
| Special Conditions | Progress on any special conditions of supervision must be reported. |
| Law Enforcement Contact | Any contact with law enforcement in the past month must be disclosed. |
| Personal Goals | Supervisees are encouraged to set personal goals and outline action steps to achieve them. |
| Signature Requirement | The report must be signed by both the supervisee and the supervising officer. |
Completing the Florida Supervision Report form is an important step in maintaining compliance with supervision requirements. After filling out the form, you will submit it to your supervising officer for review. Ensure that all sections are completed accurately to avoid any delays or issues.
What is the purpose of the Florida Supervision Report form?
The Florida Supervision Report form is designed to provide the Department of Corrections with essential information regarding an individual's compliance with the terms of their supervision. This report helps probation officers monitor progress and address any issues that may arise during the supervision period.
Who is required to complete this form?
Individuals who are currently under supervision by the Florida Department of Corrections must complete this form. It is typically filled out monthly and submitted to the supervising officer to ensure that all conditions of supervision are being met.
What information must be included in the report?
The report requires various details, including:
How often must the Florida Supervision Report be submitted?
This report must be submitted monthly. It is essential to adhere to this timeline to remain in compliance with the terms of supervision. Late submissions may lead to consequences, including a review of the individual's compliance status.
What should I do if I am unable to complete the report on time?
If you anticipate being unable to complete the report on time, it is advisable to contact your supervising officer as soon as possible. They may provide guidance or an extension, depending on the circumstances. Open communication is crucial in these situations.
Are there any attachments required with the report?
Yes, certain attachments may be required, such as proof of enrollment in educational programs, documentation of public service hours, and any required support group attendance forms. It is important to check the specific requirements for your situation.
What happens if I fail to submit the report?
Failure to submit the report can result in a violation of supervision terms. This may lead to a range of consequences, including increased scrutiny from the supervising officer, potential court hearings, or even revocation of supervision. It is crucial to prioritize timely submission of the report.
Filling out the Florida Supervision Report form can be challenging, and mistakes can lead to delays or complications. One common error is failing to provide complete and accurate personal information. This includes not filling in the full name, DC number, or contact details. Omitting any of these details can create confusion and may result in the report being rejected.
Another frequent mistake is neglecting to list all household members. The form requires the names, ages, and relationships of everyone living at the residence. If someone is on supervision, that must be noted as well. Incomplete information can hinder the review process and may affect the individual's supervision status.
People often overlook the section regarding employment. Providing inaccurate details about job title, duties, or salary can lead to misunderstandings. It is crucial to report the correct employment status, including dates and hours worked. If someone is unemployed, they must attach a job search form. Failing to do so can raise concerns about compliance with supervision requirements.
Another area where mistakes frequently occur is in documenting special conditions of supervision. Individuals need to detail their progress on public service hours, monetary payments, and any treatment attended. Incomplete or vague responses can give the impression that the individual is not taking their supervision seriously. This could lead to further scrutiny from the supervising officer.
Lastly, many individuals forget to sign the report or include the date. This simple oversight can result in the report being considered incomplete. It is essential to ensure that both the individual and the supervising officer sign and date the form to confirm that the information is accurate and reviewed. Taking the time to carefully complete the form can prevent unnecessary complications and ensure a smoother supervision process.
The Florida Supervision Report form is a critical document used in the probation process. Several other forms and documents are often required alongside it to ensure comprehensive reporting and compliance with supervision conditions. Below is a list of these documents, each accompanied by a brief description.
These documents collectively support the supervision process, ensuring that individuals comply with their conditions and maintain accountability. Proper completion and submission of each form are vital for effective monitoring and support.
The Florida Supervision Report form shares similarities with several other documents used in monitoring and reporting on individuals under supervision. Here are seven documents that are comparable, along with their specific similarities:
When filling out the Florida Supervision Report form, it is important to follow certain guidelines to ensure accuracy and compliance. Below is a list of things you should and shouldn't do:
This form is used for various types of supervision, not just probation. Individuals on parole or other forms of community supervision must also complete it.
Filling out the Supervision Report is mandatory for individuals under supervision. It helps ensure compliance with the conditions set by the court or supervising officer.
While employment is a significant part, the report also covers living conditions, personal goals, and interactions with law enforcement, among other things.
The report must be submitted by a specific deadline each month. Missing this deadline can lead to complications with your supervision.
Setting and working towards personal goals is an essential part of the supervision process. It demonstrates commitment to personal growth and rehabilitation.
Submitting an incomplete report can lead to negative consequences, including potential violations of supervision terms. It’s crucial to provide all required information.
Maintaining records of your activities, such as public service hours or treatment attendance, is essential. These documents may need to be attached to your report for verification.
Ensure that all personal information, including your name, DC number, and contact details, is accurately filled out. This information is crucial for proper identification and communication.
List all individuals currently living at your residence, noting if any are also under supervision. This helps maintain transparency regarding your living situation.
Provide comprehensive details about your employment, including your job title, duties, and salary. This information is important for monitoring your financial stability.
If you are unemployed, attach a completed Job Search form or a list of job applications for the month. This demonstrates your efforts to secure employment.
Document any special conditions of supervision, including public service hours and monetary payments. This will show your compliance with court orders.
Attach any required documentation, such as support group attendance forms or driving logs, to substantiate your claims and fulfill reporting requirements.
If you had any contact with law enforcement during the month, provide detailed explanations. This information is vital for your probation officer's review.
Set personal goals and outline specific action steps you took and will take to achieve them. This reflects your commitment to personal development and accountability.