The Florida Proof of Loss form is an essential document in the insurance claims process. It serves as a sworn statement that outlines the specifics of a loss, including the date, time, and cause of the incident. When filing a claim, the insured must provide details such as the policy number, claim number, and the total amount of insurance at the time of loss. This form requires the insured to declare their interest in the property and disclose any mortgages or lienholders. It also asks for information about any other insurance policies that may cover the same loss. Transparency is crucial; therefore, the form emphasizes that no misleading or false information should be included. The insured must certify that the details provided are accurate to the best of their knowledge. This not only helps in processing the claim efficiently but also protects against potential legal issues arising from fraudulent claims. Completing this form accurately is vital for ensuring that you receive the compensation you deserve.

| Fact Name | Description |
|---|---|
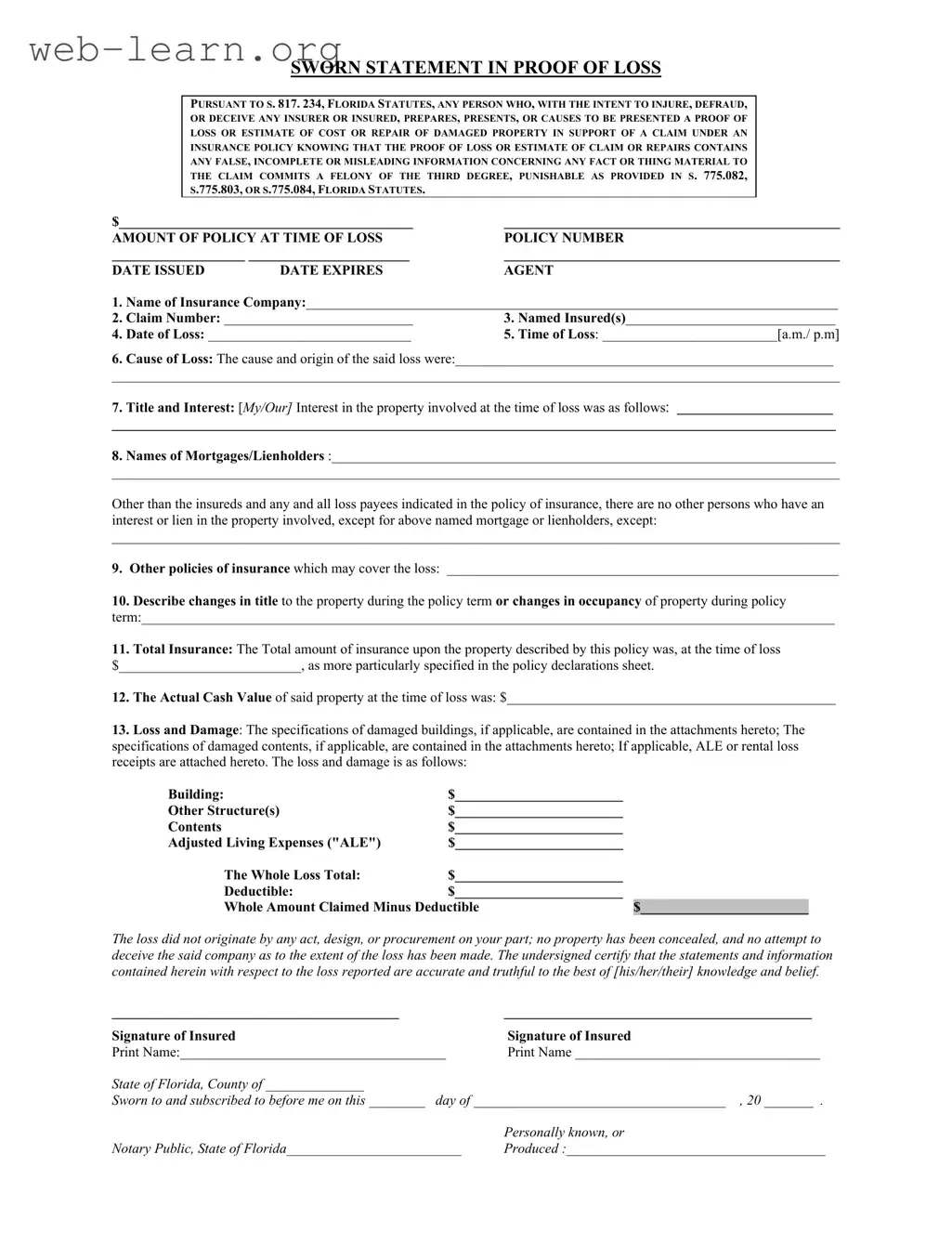
| Governing Law | The Florida Proof of Loss form is governed by Section 817.234 of the Florida Statutes. |
| Fraud Penalty | Submitting a fraudulent Proof of Loss can result in a third-degree felony charge, punishable under Sections 775.082, 775.083, or 775.084 of Florida Statutes. |
| Insurance Company Details | The form requires detailed information about the insurance company, including its name and the policy number. |
| Claim Information | It is essential to provide the claim number, date of loss, time of loss, and the cause of loss in the form. |
| Interest in Property | The form asks for the insured's interest in the property at the time of the loss, which must be clearly stated. |
| Supporting Documentation | Attachments may be required to detail the specifications of damaged buildings and contents, as well as any additional living expenses incurred. |
After completing the Florida Proof of Loss form, the next step involves submitting it to your insurance company. Ensure that all information is accurate and truthful, as any discrepancies may delay the processing of your claim.
The Florida Proof of Loss form is a legal document required by insurance companies in Florida. It serves to formally report a claim for damages or loss under an insurance policy. The form must be completed accurately and submitted to the insurer to initiate the claims process.
The form must be completed by the insured individual or entity who is filing the claim. This includes any named insureds on the policy. It is crucial that the person completing the form has a clear understanding of the details surrounding the loss.
The form requires various pieces of information, including:
Providing false, incomplete, or misleading information on the Proof of Loss form is a serious offense. Under Florida law, it is considered a felony of the third degree. This could lead to severe legal consequences, including fines and imprisonment.
The Actual Cash Value (ACV) of the property at the time of loss is determined by assessing the market value of the property, taking into account depreciation. This value is essential for calculating the amount of the claim and should be documented accurately on the form.
A notary public is required to witness the signing of the Proof of Loss form. This adds a layer of authenticity to the document, ensuring that the signatures are valid and that the information provided is sworn to be true.
Yes, it is often advisable to submit additional documents that support your claim. This may include receipts for damaged property, photographs of the loss, and any relevant repair estimates. Attach these documents to the Proof of Loss form to provide a comprehensive view of your claim.
If you have questions while filling out the form, it is recommended to contact your insurance agent or the claims department of your insurance company. They can provide guidance and clarify any uncertainties you may have.
The timeframe for submitting the Proof of Loss form can vary by insurance policy. Typically, it is advisable to submit the form as soon as possible after the loss occurs. Check your policy for specific deadlines to ensure compliance.
After submitting the Proof of Loss form, it is important to keep a copy for your records. Follow up with your insurance company to confirm receipt and inquire about the next steps in the claims process. Stay in communication with your insurer to ensure a smooth resolution.
Filling out the Florida Proof of Loss form can be a straightforward process, but many people make common mistakes that can complicate their claims. One significant error is failing to provide complete information. Each section of the form requires specific details, such as the date and time of loss, the cause of loss, and the total insurance amount. Omitting even one detail can lead to delays or denials.
Another frequent mistake is misrepresenting the value of the damaged property. It is essential to accurately state the Actual Cash Value at the time of loss. Underestimating or overestimating this value can have serious implications for the claim. Insurers rely on this information to assess the legitimacy of the claim.
People often neglect to include all relevant parties in the claim. If there are any mortgages or lienholders, they must be listed on the form. Failure to disclose this information can result in complications, as the insurer may need to address the interests of these parties before processing the claim.
Some individuals do not attach supporting documentation to the form. This documentation can include estimates for repairs, receipts for damaged contents, and any other relevant evidence. Without these attachments, the claim may lack the necessary support to be processed efficiently.
Another common oversight is failing to sign the form correctly. Both insured parties must provide their signatures, and any missing signatures can halt the claims process. Additionally, the form must be notarized to confirm its authenticity, which is often overlooked.
Misunderstanding the deductible can lead to confusion as well. Claimants should clearly state the deductible amount and ensure it is accurately reflected in the total amount claimed. Not doing so can result in discrepancies that delay payment.
Lastly, people sometimes submit the form without thoroughly reviewing it for accuracy. Errors in spelling, numbers, or factual information can undermine the credibility of the claim. A careful review can prevent these mistakes and facilitate a smoother claims process.
By avoiding these common pitfalls, individuals can increase their chances of a successful claim. Attention to detail is crucial when filling out the Florida Proof of Loss form.
The Florida Proof of Loss form is essential for filing an insurance claim. However, several other documents may also be required to support your claim effectively. Below is a list of forms and documents that are often used in conjunction with the Florida Proof of Loss form, along with brief descriptions of each.
Gathering these documents can help ensure a smoother claims process. Being thorough and organized will support your case and may expedite the resolution of your claim.
The Florida Proof of Loss form serves as a critical document in the insurance claims process, specifically for reporting losses and damages to an insurer. Several other documents share similarities with this form, each serving its unique purpose but often requiring comparable information. Below is a list of ten documents that are similar to the Florida Proof of Loss form:
When filling out the Florida Proof of Loss form, there are several important considerations to keep in mind. Here’s a list of what you should and shouldn’t do:
Understanding the Florida Proof of Loss form is crucial for policyholders. However, several misconceptions exist regarding its use and implications. Here are ten common misconceptions:
Being aware of these misconceptions can help policyholders navigate the claims process more effectively and ensure compliance with their insurance requirements.