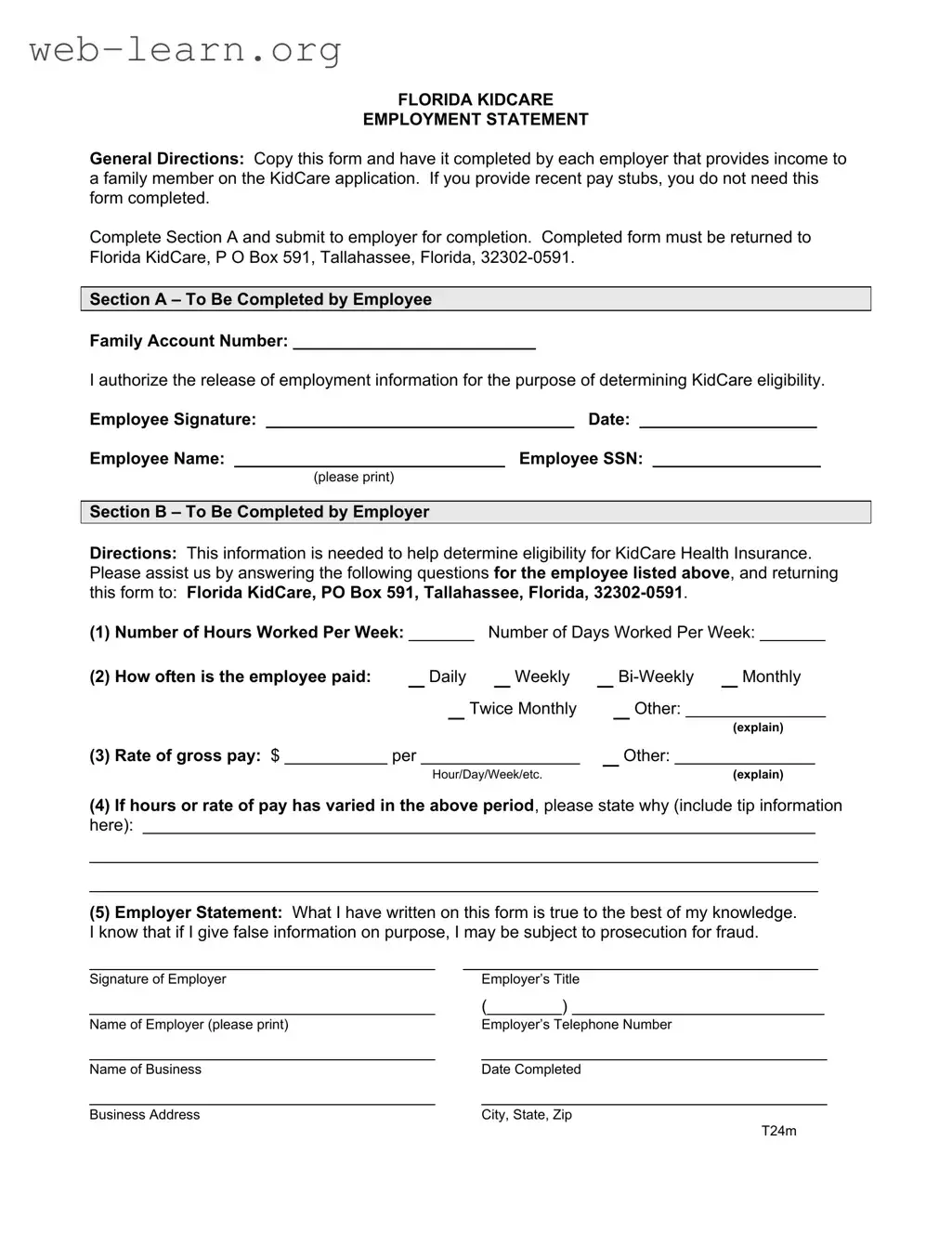
The Florida KidCare form is an essential document for families seeking health insurance coverage for their children. It plays a crucial role in the application process by gathering necessary employment information from family members. To complete this form, employers must provide details about the employee's work hours, pay frequency, and gross pay rate. If recent pay stubs are available, the form is not required. The form consists of two main sections: Section A, completed by the employee, where they authorize the release of their employment information; and Section B, filled out by the employer, which includes specific questions about the employee's work situation. Once completed, the form must be sent to Florida KidCare in Tallahassee, ensuring that the information is accurate and truthful to avoid any potential issues with eligibility. Understanding the requirements of this form is vital for families to secure the health insurance benefits their children need.
| Fact Name | Fact Details |
|---|---|
| Purpose | The Florida KidCare Employment Statement is used to verify income for families applying for KidCare health insurance. |
| Completion Requirement | Employers must complete the form if the applicant does not provide recent pay stubs. |
| Submission Address | Completed forms must be sent to Florida KidCare, P.O. Box 591, Tallahassee, Florida, 32302-0591. |
| Section A | This section is for the employee to authorize the release of employment information. |
| Section B | Employers fill out this section to provide necessary details about the employee's work hours and pay. |
| Legal Authority | The form is governed by Florida Statutes, Chapter 409, which pertains to public assistance programs. |
| Fraud Warning | Employers are warned that providing false information may lead to prosecution for fraud. |
| Employer Information | Employers must provide their name, title, business name, and contact information on the form. |
After gathering the necessary information, the next step is to complete the Florida KidCare form accurately. This form is essential for determining eligibility for health insurance coverage for children. Follow the steps below to ensure that the form is filled out correctly.
What is the purpose of the Florida KidCare Employment Statement?
The Florida KidCare Employment Statement is a form used to gather employment information for individuals applying for KidCare health insurance. This information helps determine eligibility for the program. If recent pay stubs are provided, this form is not necessary.
Who needs to complete the Florida KidCare Employment Statement?
Each employer that provides income to a family member on the KidCare application must complete the form. The employee must fill out Section A and submit it to their employer for completion of Section B.
How should the completed form be submitted?
The completed Florida KidCare Employment Statement must be returned to Florida KidCare at the following address:
P.O. Box 591,
Tallahassee, Florida, 32302-0591.
What information is required from the employee?
In Section A, the employee must provide their family account number, authorize the release of employment information, and sign the form. Additionally, the employee's name and Social Security Number must be printed on the form.
What details does the employer need to provide?
Section B requires the employer to provide specific information including:
This information is crucial for accurately assessing the employee's eligibility for KidCare.
What happens if false information is provided?
Employers must certify that the information they provide is true to the best of their knowledge. If false information is given intentionally, the employer may face prosecution for fraud.
Is there a deadline for submitting the form?
While the form does not specify a deadline, it is advisable to submit it as soon as possible to avoid delays in the eligibility determination process for KidCare health insurance.
When filling out the Florida KidCare form, individuals often encounter several common mistakes that can lead to delays in processing or even denial of eligibility. Understanding these pitfalls can help ensure a smoother application experience.
One frequent error is incomplete information. Applicants sometimes neglect to fill out all required fields, particularly in Section A. Missing details such as the Family Account Number or the Employee Signature can result in the form being returned. It’s essential to double-check that every section is filled out completely before submission.
Another common mistake involves incorrect employment information. Employers must provide accurate data regarding hours worked and pay rates. If an employee works variable hours or has fluctuating pay, this should be clearly explained in the designated section. Failing to provide this context can lead to misunderstandings about the employee's income and may impact eligibility.
Additionally, applicants often overlook the importance of signatures. Both the employee and employer must sign the form. If either signature is missing, the application will not be processed. It is advisable to confirm that both parties have signed and dated the form before sending it off to Florida KidCare.
Some individuals may also misinterpret the payment frequency section. It is crucial to select the correct option—whether it is daily, weekly, bi-weekly, or monthly. Misrepresenting how often the employee is paid can lead to discrepancies in income calculations, which may affect the overall eligibility assessment.
Finally, failing to submit the form to the correct address can cause significant delays. The completed form must be sent to Florida KidCare at the specified P.O. Box in Tallahassee. Ensuring that the mailing address is accurate and complete is vital for timely processing.
When applying for Florida KidCare, several forms and documents may be required to support your application. Each of these documents plays a crucial role in ensuring eligibility for the program. Here’s a list of commonly used forms that you might encounter.
Gathering these documents ahead of time can streamline the application process and help ensure that your family receives the necessary coverage without unnecessary delays. Make sure to keep copies of everything you submit for your records.
The Florida KidCare Employment Statement is a specific form designed to gather employment information for determining eligibility for health insurance coverage. Several other documents serve similar purposes in different contexts. Below is a list of documents that share similarities with the Florida KidCare form:
When filling out the Florida KidCare form, it is crucial to follow specific guidelines to ensure the process goes smoothly. Here are some dos and don'ts to keep in mind:
There are several misconceptions surrounding the Florida KidCare form that can lead to confusion. Understanding these misconceptions can help ensure a smoother application process for families seeking health insurance coverage for their children.
When filling out and using the Florida KidCare form, it's essential to keep a few key points in mind. Here are five important takeaways: