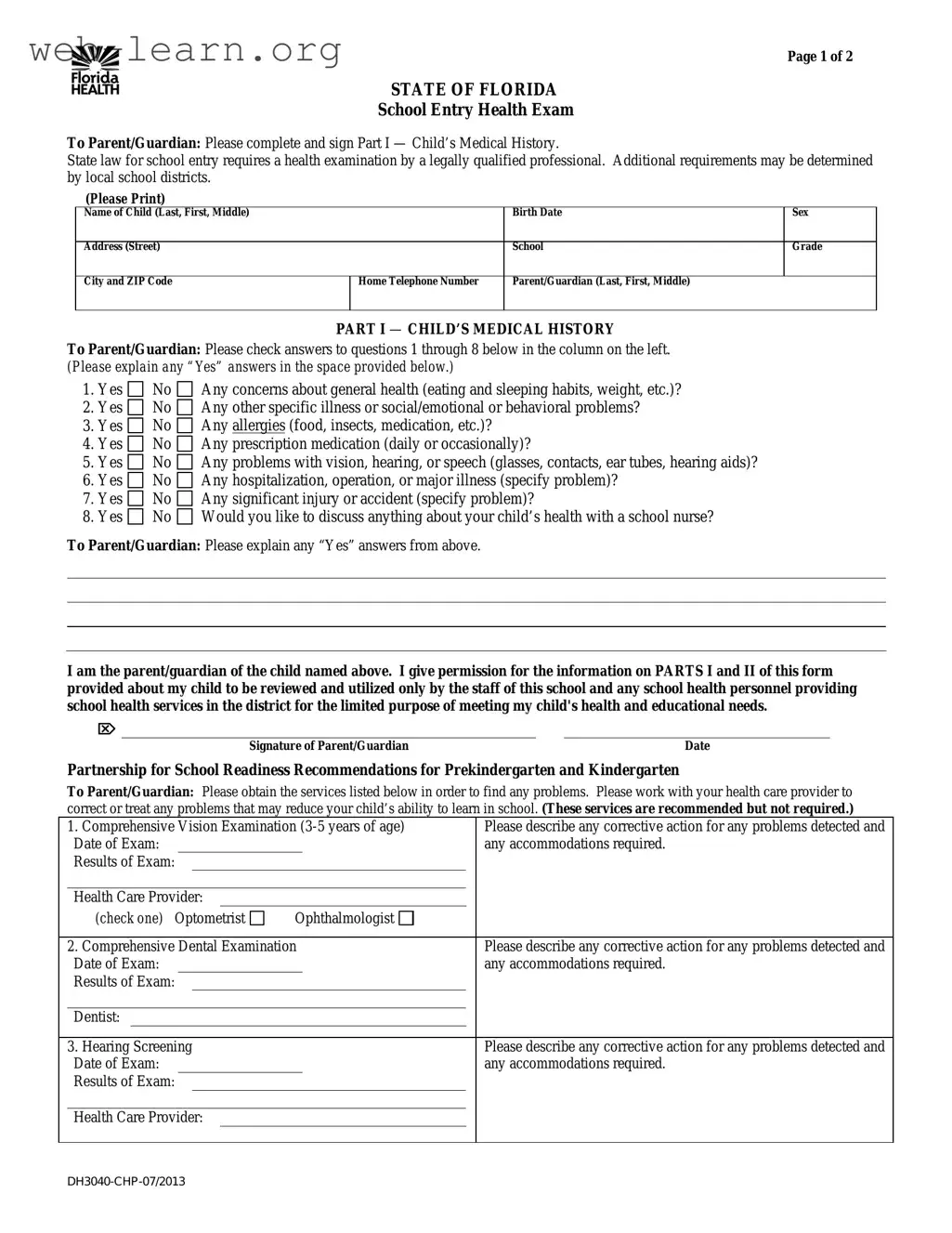
The Florida Health form is an essential document for parents and guardians as their children prepare to enter school. This form is designed to collect vital information regarding a child's medical history, ensuring that schools can adequately address their health needs. Parents must complete Part I, which includes questions about general health, allergies, and any existing medical conditions that may affect the child's learning experience. Additionally, it provides space to elaborate on any "Yes" answers, allowing for a comprehensive understanding of the child's health status. Part II requires a licensed health care provider to conduct a thorough medical evaluation, including a physical exam and screenings for vision, hearing, and other health indicators. This section also highlights any health conditions that may necessitate special accommodations at school. Furthermore, the form emphasizes the importance of follow-up services, such as dental and vision examinations, to support the child's overall well-being and readiness for school. By completing this form, parents play a crucial role in fostering a safe and supportive educational environment for their children.
| Fact Name | Description |
|---|---|
| Purpose of the Form | This form is required for school entry in Florida. It collects important health information about the child to ensure their well-being and ability to learn. |
| Legal Requirement | Florida law mandates that a health examination be conducted by a qualified professional before a child can enter school. |
| Parental Consent | Parents or guardians must sign the form, granting permission for the school staff to use the health information provided for educational needs. |
| Additional Recommendations | The form suggests obtaining additional health services, such as vision and dental exams, to address any potential issues affecting the child's learning. |
Completing the Florida Health form is an essential step for ensuring your child’s health needs are documented for school entry. This process involves gathering important medical information and having a qualified health care provider complete a medical evaluation. Follow these steps carefully to fill out the form accurately.
What is the purpose of the Florida Health form?
The Florida Health form is required for school entry and ensures that children receive a comprehensive health examination by a qualified professional. This form collects important medical history and current health information to help school staff support the child's health and educational needs.
Who needs to fill out the form?
The form must be completed by the child's parent or guardian. It is crucial that they provide accurate information about the child's medical history, including any health concerns, allergies, or medications.
What information is required in Part I of the form?
Part I includes questions regarding the child's general health, specific illnesses, allergies, medications, and any issues related to vision, hearing, or speech. Parents should check “Yes” or “No” for each question and provide explanations for any “Yes” answers.
What should I do if my child has a medical condition?
If your child has a health condition that may require special attention at school, you must specify this in the form. This includes conditions like allergies or seizures. The information will be stored in the child’s Cumulative Health Folder and will be accessible to school and health personnel.
Are there any additional health services recommended?
Yes, the form recommends several services, such as a comprehensive vision examination, dental examination, and hearing screening. While these services are not mandatory, they are encouraged to help identify any issues that could affect your child's learning.
What happens in Part II of the form?
Part II must be completed by a health care provider. This section includes a complete history and physical exam, along with screening results like height, weight, and vision. The provider will also indicate any health conditions that could impact the child’s educational experience.
How is the information on the form used?
The information provided on the Florida Health form is used solely for the purpose of meeting the child's health and educational needs. School staff and health personnel will review the data to ensure appropriate support and accommodations are in place for the child.
When filling out the Florida Health form, many parents and guardians make common mistakes that can lead to delays or complications. One frequent error is failing to provide complete information in the child's medical history. Each question in Part I requires careful consideration. If a parent checks "Yes" for any health concerns, they must provide detailed explanations. Omitting this information can hinder the school’s ability to support the child's health needs.
Another mistake involves incorrect or incomplete contact information. The form requires accurate details such as the child's name, address, and parent/guardian contact numbers. If any of these fields are left blank or filled out incorrectly, it can create challenges in communication between the school and the family, especially in emergencies.
Parents also often overlook the importance of having the health care provider complete Part II of the form. This section is crucial as it includes the child's physical examination results and any health conditions that may affect their school experience. If this part is missing or improperly filled out, the school may not have the necessary information to ensure the child's safety and well-being.
Additionally, many individuals neglect to check for updates on local school district requirements. While the state mandates certain health examinations, local districts may have additional criteria. Failing to comply with these can result in the child being unable to enroll or participate in school activities.
Finally, parents sometimes forget to sign and date the form. A signature is required to authorize the use of the health information provided. Without it, the form is incomplete and may not be accepted by the school. Each of these mistakes can lead to significant delays in processing the health form, ultimately affecting the child’s school entry and health services.
When completing the Florida Health form for school entry, several additional documents may be necessary to ensure a comprehensive understanding of your child's health needs. Below are some commonly used forms that complement the Florida Health form.
Having these documents ready can facilitate a smoother enrollment process and help ensure that your child's health and educational needs are adequately addressed. It is always advisable to consult with your healthcare provider or school nurse if you have any questions regarding these forms.
When filling out the Florida Health form, there are several important dos and don’ts to keep in mind. Following these guidelines will help ensure that the process goes smoothly and that your child's health information is accurately represented.
Misconceptions about the Florida Health form can lead to confusion for parents and guardians. Here are ten common misunderstandings, along with clarifications:
Understanding these misconceptions can help parents navigate the process more effectively and ensure their child's health needs are met.
Filling out the Florida Health form is an important step for your child's school entry. Here are some key takeaways to keep in mind: