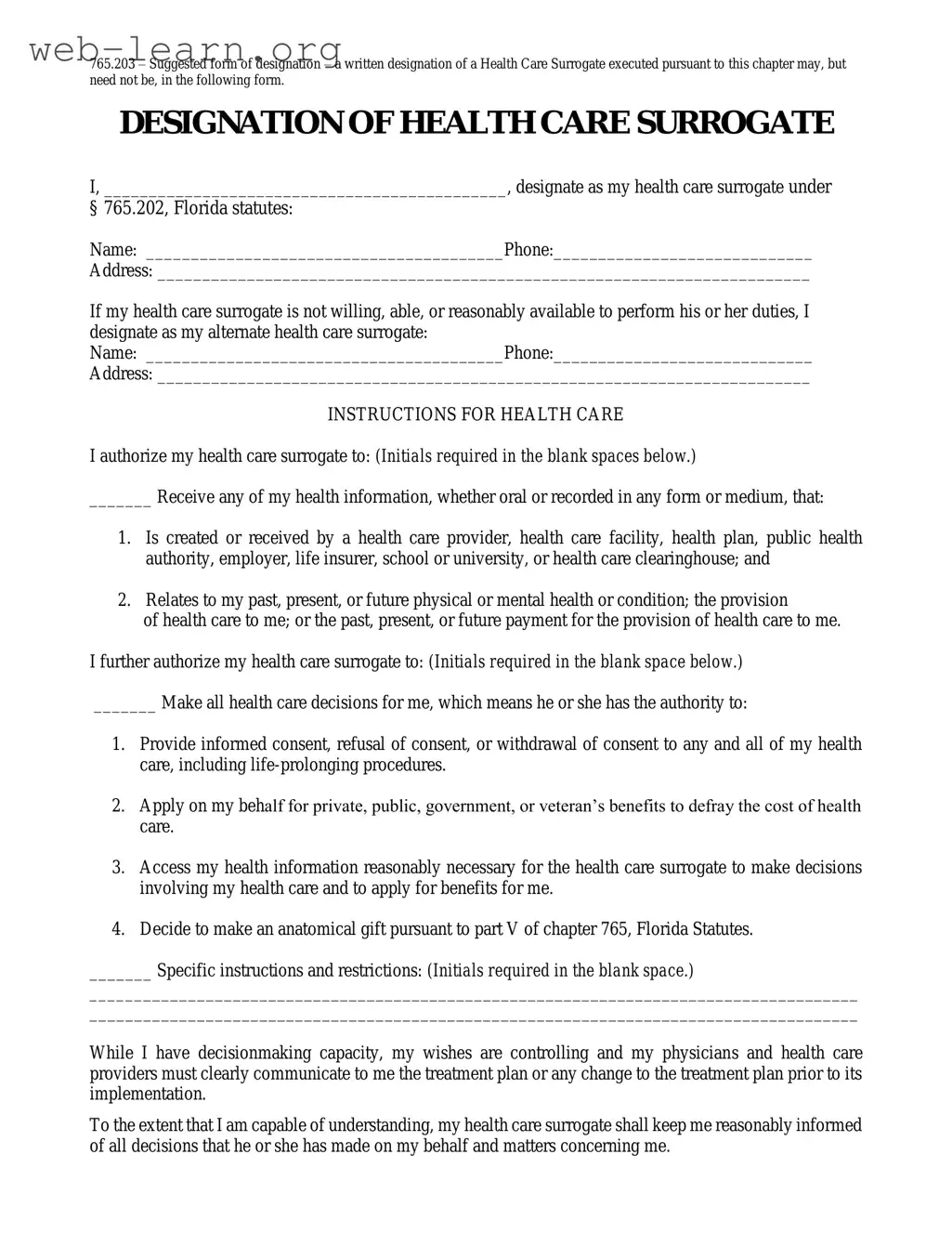
The Florida Health Care Surrogate form is an essential legal document that allows individuals to designate a trusted person to make health care decisions on their behalf in the event they become unable to do so. This form requires the designation of a primary health care surrogate, along with an alternate in case the primary is unavailable or unwilling to serve. It outlines the authority granted to the surrogate, which includes accessing medical information, providing informed consent, and making decisions regarding medical treatment, including life-prolonging procedures. The form also allows for specific instructions and restrictions to be included, ensuring that the individual's wishes are respected. Importantly, the authority of the health care surrogate becomes effective only when a physician determines that the individual is unable to make their own health care decisions. Individuals retain the right to revoke or amend this designation while they have decision-making capacity, providing flexibility and control over their health care preferences. Understanding the implications of this form is crucial for anyone considering their health care options and the role of their surrogate.


| Fact Name | Details |
|---|---|
| Governing Law | This form is governed by Chapter 765 of the Florida Statutes. |
| Designation | Individuals can designate a health care surrogate to make medical decisions on their behalf. |
| Alternate Surrogate | An alternate health care surrogate can be named if the primary is unavailable. |
| Health Information Access | The surrogate is authorized to receive all health information related to the individual. |
| Decision-Making Authority | The surrogate has the authority to make informed consent decisions regarding health care. |
| Revocation | Individuals can revoke or amend their designation while retaining decision-making capacity. |
| Effective Date | The surrogate's authority becomes effective when a physician determines the individual is unable to make their own decisions. |
Filling out the Florida Health Care Surrogate form is a straightforward process. This document allows you to designate someone to make health care decisions on your behalf if you are unable to do so. To ensure that your wishes are clearly communicated, follow these steps carefully.
After completing the form, keep it in a safe place and consider sharing copies with your health care surrogate and your primary physician. This will help ensure that your health care wishes are respected when the time comes.
The Florida Health Care Surrogate form is a legal document that allows an individual to designate another person to make health care decisions on their behalf if they become unable to do so. This designation ensures that someone the individual trusts will be responsible for making important medical choices in line with their wishes.
Any adult can serve as a health care surrogate, provided they are willing and able to take on this responsibility. It is important to choose someone who understands your values and preferences regarding medical treatment. This person can be a family member, a close friend, or anyone you trust.
A health care surrogate has the authority to make a wide range of health care decisions, including:
Yes, the Florida Health Care Surrogate form allows you to include specific instructions or restrictions regarding your health care. This can guide your surrogate in making decisions that align with your personal values and preferences.
The authority of your health care surrogate typically becomes effective when your primary physician determines that you are unable to make your own health care decisions. However, you can choose to have their authority take effect immediately by initialing the appropriate box on the form.
Yes, you can revoke or amend the designation at any time while you still have decision-making capacity. This can be done by signing a new document, verbally expressing your intent, or physically destroying the original document in the presence of another person.
If you regain the ability to make your own decisions, your wishes will take precedence over those of your health care surrogate. This means that any health care decisions you make while capable will override any conflicting decisions made by your surrogate.
Yes, the Florida Health Care Surrogate form requires the signatures of two witnesses. These witnesses must be adults who are not related to you and who will not benefit from your estate. Their signatures help validate the document and ensure it meets legal requirements.
No, the designation is not permanent. It remains in effect until you revoke it or until your health care surrogate is no longer able to serve. You can change your surrogate or the terms of your designation as your circumstances or preferences change.
Filling out the Florida Health Care Surrogate form can be a straightforward process, but there are common mistakes that individuals often make. These errors can lead to complications when the time comes to implement the designated health care surrogate's authority. Understanding these pitfalls can help ensure that your wishes are honored.
One common mistake is failing to provide complete information about the health care surrogate. It's crucial to include the surrogate's full name, phone number, and address. Omitting any of this information can create confusion and may result in delays when urgent health care decisions need to be made. A health care surrogate should be someone who can be easily contacted and who understands your wishes.
Another frequent error involves not designating an alternate health care surrogate. Life is unpredictable, and your first choice may not always be available to make decisions on your behalf. By failing to name an alternate, you risk leaving your health care decisions in limbo, which can be distressing for both you and your loved ones.
Many people also neglect to initial the required sections that grant their health care surrogate specific powers. This step is not merely a formality; it indicates your consent for the surrogate to access your health information and make decisions regarding your care. Without these initials, the surrogate may not have the authority to act when needed.
Additionally, some individuals mistakenly believe that their health care surrogate's authority is automatically effective upon signing the form. However, the authority typically only becomes effective when a primary physician determines that the individual is unable to make their own health care decisions. Failing to understand this can lead to misunderstandings about when the surrogate can step in.
Another mistake is not communicating specific instructions or restrictions clearly. If there are particular wishes regarding medical treatment or interventions, they should be explicitly stated on the form. Vague instructions can lead to confusion and may not reflect your true desires when decisions need to be made.
People often overlook the importance of having witnesses sign the form. The signatures of two witnesses are generally required to validate the document. Without these signatures, the form may be deemed invalid, which can complicate matters when your health care surrogate needs to act on your behalf.
Finally, many individuals forget to keep a copy of the completed form in an accessible location. It’s essential to ensure that your health care surrogate and close family members know where to find it. If the form cannot be located when needed, it can create unnecessary stress during an already challenging time.
By being aware of these common mistakes, individuals can take proactive steps to ensure that their Florida Health Care Surrogate form accurately reflects their wishes and is legally valid. This careful attention to detail can provide peace of mind, knowing that your health care decisions will be honored when it matters most.
The Florida Health Care Surrogate form is an important document that allows individuals to designate someone to make health care decisions on their behalf if they become unable to do so. Along with this form, several other documents can complement or enhance its effectiveness. Here are a few commonly used forms:
Each of these documents serves a unique purpose and can work together to ensure that an individual's health care preferences are respected. It's essential to consider these options carefully and discuss them with loved ones and health care providers.
When filling out the Florida Health Care Surrogate form, there are important dos and don'ts to keep in mind. This will help ensure that your wishes are respected and that the process goes smoothly.
Understanding the Florida Health Care Surrogate form is crucial for anyone considering designating a surrogate for health care decisions. However, several misconceptions often arise. Here are ten common misunderstandings along with clarifications:
This form is beneficial for anyone over the age of 18, regardless of health status. It allows individuals to designate someone they trust to make medical decisions on their behalf if they become incapacitated.
The authority of a health care surrogate only activates when the primary physician determines that the individual is unable to make their own health care decisions. Until that point, the individual retains full decision-making capacity.
Individuals can revoke or amend the designation at any time while they have decision-making capacity. This can be done through a written statement, destruction of the form, or verbal expression of intent.
The individual's wishes take precedence. If they have decision-making capacity, their instructions must be followed, even if they conflict with the surrogate's decisions.
The Florida Health Care Surrogate form can be completed without legal assistance. It is designed to be straightforward and accessible for all individuals.
Two witnesses are required to sign the form for it to be legally binding. These witnesses must be present when the individual signs the document.
While many people choose family members, the surrogate can be anyone the individual trusts, including friends or other trusted individuals, as long as they are over 18.
The surrogate's authority is limited to health care decisions only. They cannot make financial or legal decisions unless specifically authorized in a separate document.
The form is useful for any situation where an individual might become unable to make health care decisions, not just in terminal cases. This includes accidents or sudden illnesses.
It is advisable to discuss the designation with the chosen surrogate and family members. Open communication ensures everyone understands the individual's wishes and the surrogate's role.
Addressing these misconceptions can help individuals make informed decisions about their health care preferences and ensure their wishes are respected when they cannot advocate for themselves.
Here are some key takeaways about filling out and using the Florida Health Care Surrogate form: