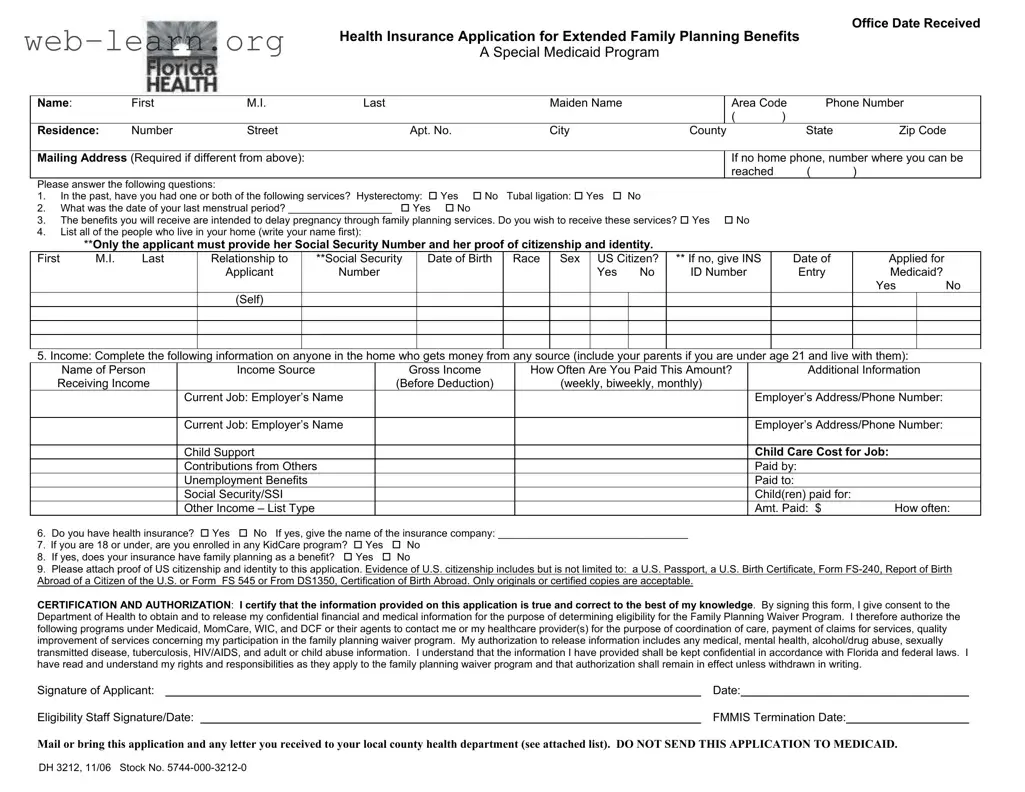
The Florida DH 3212 form is an essential document designed to facilitate access to extended family planning benefits under a special Medicaid program. This application is specifically tailored for individuals who have lost full Medicaid coverage and are seeking family planning services to help delay pregnancy. To initiate the process, applicants must provide personal information, including their name, contact details, and residence. The form also requires responses to several questions regarding reproductive history, such as whether the applicant has undergone a hysterectomy or tubal ligation, as well as their last menstrual period. Additionally, the form gathers information about household members, their income sources, and any existing health insurance coverage. It is crucial for applicants to attach proof of U.S. citizenship and identity, as well as to sign a certification that allows the Department of Health to access necessary confidential information. Understanding the requirements and completing the DH 3212 accurately can significantly impact eligibility for the Medicaid Family Planning Waiver program, which is aimed at individuals with specific income thresholds and family planning needs.

| Fact Name | Details |
|---|---|
| Form Purpose | The Florida DH 3212 form is used to apply for extended family planning benefits under Medicaid. |
| Eligibility Criteria | Applicants must have lost full Medicaid, not have had a hysterectomy or tubal ligation, not be pregnant, desire family planning services, and have an income at or below 185% of the federal poverty level. |
| Required Information | Applicants must provide personal information, reproductive history, and details about household members and their income. |
| Proof of Citizenship | Only the applicant must submit proof of U.S. citizenship and identity, such as a U.S. passport or birth certificate. |
| Health Insurance Inquiry | Applicants are asked whether they have health insurance and if family planning is a covered benefit. |
| Signature Requirement | The applicant must sign and date the form to certify the information provided is accurate. |
| Submission Instructions | The completed form must be mailed or delivered to the local county health department, not Medicaid. |
| Confidentiality | The information provided will be kept confidential according to Florida and federal laws. |
| Governing Law | The form is governed by Florida Statutes related to Medicaid and family planning services. |
| Form Version | The current version of the form is dated November 2006. |
Completing the Florida DH 3212 form is a crucial step in applying for extended family planning benefits through Medicaid. After filling out the form, you will need to submit it to your local county health department for processing. Ensure that all required information is accurately provided to avoid delays in your application.
What is the purpose of the Florida DH 3212 form?
The Florida DH 3212 form is used to apply for the Health Insurance Application for Extended Family Planning Benefits, which is a special Medicaid program. This program aims to provide family planning services to eligible individuals who have lost their full Medicaid coverage. It helps individuals access necessary services to delay pregnancy and manage reproductive health effectively.
Who is eligible to apply for the Family Planning Waiver Program?
To be eligible for the Family Planning Waiver Program, applicants must meet specific criteria:
Meeting these requirements is essential for successful application and approval.
What information do I need to provide on the form?
The form requires various personal details, including:
Only the applicant needs to provide their Social Security Number and proof of U.S. citizenship and identity. This information is crucial for determining eligibility.
How do I submit the DH 3212 form?
Once you have completed the form, it should not be sent to Medicaid directly. Instead, you must mail or bring the application to your local county health department. It is important to ensure that all sections of the form are filled out accurately to avoid delays in processing your application.
Filling out the Florida DH 3212 form can be a crucial step in securing family planning benefits. However, many people make common mistakes that can delay their application. One frequent error is not providing complete contact information. It’s essential to include both your residence and mailing addresses. If these differ, omitting the mailing address can lead to missed communications regarding your eligibility.
Another mistake involves answering the questions inaccurately or incompletely. For instance, when asked about previous medical procedures like a hysterectomy or tubal ligation, be sure to answer honestly. Misrepresenting your medical history can jeopardize your application. Additionally, many applicants forget to provide the date of their last menstrual period, which is a critical piece of information for determining eligibility.
Providing insufficient information about household members is another common pitfall. When listing everyone who lives in your home, ensure you include all required details, such as Social Security numbers and dates of birth. This information is vital for assessing household income and eligibility. Also, remember that only the applicant needs to provide proof of citizenship and identity, but this must be done correctly with certified copies or originals.
Income reporting can also be tricky. Applicants often fail to include all sources of income for everyone in the household. This includes child support, unemployment benefits, and any other financial contributions. Make sure to detail how often you receive this income, as this information plays a significant role in determining eligibility for the program.
Another mistake is neglecting to check the health insurance questions thoroughly. If you do have health insurance, you must provide the name of the insurance company. Forgetting to answer these questions can lead to unnecessary delays in processing your application.
Many applicants overlook the importance of signing and dating the form. The certification section confirms that you understand the information provided is accurate. Failing to sign can result in the application being returned or rejected.
Lastly, it’s crucial to remember where to send the application. Some people mistakenly send their forms to Medicaid instead of their local county health department. This misdirection can significantly delay the review process.
By avoiding these common mistakes, you can help ensure a smoother application process for the Florida DH 3212 form and increase your chances of receiving the benefits you need.
The Florida DH 3212 form is part of the application process for the Medicaid Family Planning Waiver Program. Several other forms and documents are often required or recommended to accompany this application. Below is a list of commonly used documents that may assist in the application process.
Gathering these documents can streamline the application process for the Florida DH 3212 form. Proper documentation ensures that eligibility is assessed accurately and efficiently, reducing potential delays in receiving benefits.
When filling out the Florida DH 3212 form, there are several important guidelines to follow. Below is a list of things you should and shouldn't do.
Misconceptions about the Florida DH 3212 form can lead to confusion and delays in receiving benefits. Here are seven common misconceptions, along with clarifications:
Understanding these misconceptions can help streamline the application process and ensure that applicants receive the benefits they need in a timely manner.
Filling out the Florida DH 3212 form is an important step for those seeking extended family planning benefits through Medicaid. Here are some key takeaways to help you navigate the process:
Understanding these key points can streamline your application process and help ensure you receive the benefits you need. Take your time to gather the required information and complete the form accurately.