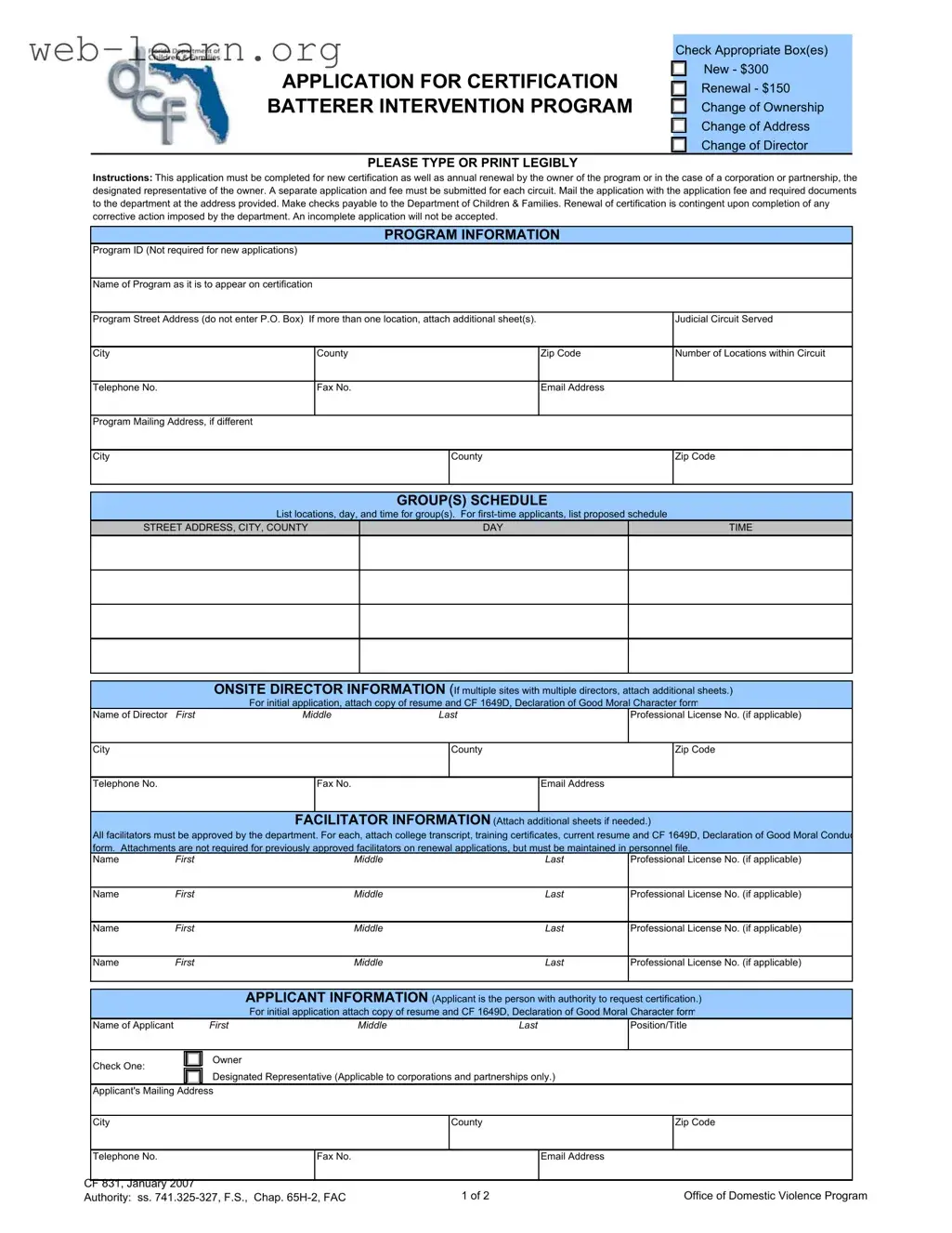
The Florida CF 831 form serves as a crucial application for certification related to Batterer Intervention Programs (BIPs) within the state. This form is necessary for both new certifications and annual renewals, with fees set at $300 for new applicants and $150 for renewals. Applicants must complete the form legibly, ensuring all required documentation accompanies the submission. It is imperative to note that each circuit requires a separate application and fee. The form collects essential information, including program details, the judicial circuit served, and the names and qualifications of onsite directors and facilitators. For initial applications, supporting documents such as resumes and declarations of good moral character are mandatory. Additionally, the form emphasizes the legal ownership structure of the program, whether it be an individual, corporation, or partnership, and requires appropriate documentation for each category. A critical aspect of the application process is adherence to state standards, as any omissions or inaccuracies can lead to rejection or suspension of certification. By submitting the CF 831 form, applicants affirm their commitment to comply with all relevant regulations governing the operation of certified programs, underscoring the importance of transparency and accountability in addressing domestic violence issues in Florida.

| Fact Name | Details |
|---|---|
| Purpose | The CF 831 form is used for applying for certification of Batterer Intervention Programs in Florida. |
| Application Types | It includes options for new applications, renewals, and changes of ownership, address, or director. |
| Fees | The fee for a new application is $300, while a renewal costs $150. |
| Submission Requirements | Each application must be completed fully and submitted with the appropriate fee and required documents. |
| Governing Laws | This form operates under Florida Statutes sections 741.325-327 and Chapter 65H-2 of the Florida Administrative Code. |
| Incomplete Applications | Any incomplete application will not be accepted by the Department of Children & Families. |
| Certification Duration | Certification is valid for one year and is non-transferable. |
| Legal Consequences | Providing false information on the application can lead to legal penalties, including misdemeanor charges. |
Completing the Florida CF 831 form is a necessary step for those seeking certification for a Batterer Intervention Program. This process involves providing detailed information about the program, its directors, facilitators, and ownership structure. The form must be filled out accurately and submitted along with the appropriate fees and supporting documents to ensure a smooth certification process.
What is the purpose of the Florida CF 831 form?
The Florida CF 831 form is used to apply for certification of a Batterer Intervention Program (BIP). This form is necessary for both new applications and annual renewals. It ensures that the program meets the standards set by the Department of Children and Families in Florida.
What fees are associated with the CF 831 form?
There are specific fees that must be submitted with the application. For new certifications, the fee is $300. If you are renewing an existing certification, the fee is $150. Make sure to include the correct payment when you send in your application.
What information is required for the application?
The application requires detailed information about the program, including:
Each section must be filled out completely. Incomplete applications will not be accepted.
How do I submit the CF 831 form?
Once you have completed the form and gathered all required documents, mail the application along with the application fee to the address provided by the Department of Children and Families. Ensure that checks are made payable to the Department of Children & Families.
What happens if my application is incomplete?
If your application is incomplete, it will be rejected. To avoid this, double-check that all sections are filled out and that you have included all necessary attachments. This includes resumes, declarations of good moral character, and any required certifications for facilitators.
Filling out the Florida CF 831 form can be a straightforward process, but many applicants make common mistakes that can delay their certification. One frequent error is failing to check the appropriate box for the type of application. Whether it’s a new application, renewal, or a change of ownership, selecting the correct option is essential. Without this initial step, the application may be rejected.
Another common mistake is neglecting to provide complete program information. It’s crucial to include the program's name, street address (not a P.O. Box), and the judicial circuit served. Omitting any of these details can lead to an incomplete application, which will not be accepted.
Many applicants also overlook the requirement to provide a mailing address if it differs from the program's street address. This oversight can create confusion and delay communication from the Department of Children and Families.
In the section for onsite director information, applicants sometimes fail to attach the necessary documents, such as a resume and the CF 1649D, Declaration of Good Moral Character form. This documentation is mandatory for initial applications and skipping it can result in rejection.
Facilitator information is another area where mistakes frequently occur. All facilitators must be approved by the department, and applicants often forget to include required attachments like college transcripts and training certificates. These documents are essential for the approval process.
When filling out the applicant information, it’s important to accurately identify the applicant's position or title. Failing to do so can lead to misunderstandings about who is responsible for the application.
Another common error involves the legal ownership section. Applicants must complete only one of the categories listed—individual, corporation, or partnership. Confusion in this area can lead to incomplete submissions.
Additionally, applicants sometimes forget to provide the required financial information, such as the FEID number and business license numbers. This information is vital for verifying the legitimacy of the program.
Finally, many applicants do not read the declaration statement carefully. It is important to understand that any misstatements can lead to serious consequences, including rejection or suspension of certification. Ensuring that all information is accurate and truthful is paramount.
The Florida CF 831 form is essential for the certification of Batterer Intervention Programs. However, there are several other forms and documents that are commonly used in conjunction with it. Each of these documents serves a specific purpose in the certification process and ensures compliance with state regulations. Below is a list of these important documents.
Each of these documents plays a vital role in the certification process for Batterer Intervention Programs in Florida. Ensuring that all forms are complete and accurate is essential for a successful application. Take prompt action to gather these documents to facilitate a smooth certification process.
The Florida CF 831 form is an important document for those seeking certification for a Batterer Intervention Program. Several other forms serve similar purposes in different contexts. Here’s a list of seven documents that share similarities with the CF 831 form:
When filling out the Florida CF 831 form, it's essential to approach the task with care and attention to detail. Here are ten important dos and don'ts to keep in mind:
By following these guidelines, you can help ensure a smoother application process and increase the likelihood of receiving certification for your batterer intervention program.
Here are nine common misconceptions about the Florida CF 831 form:
Understanding these misconceptions can help ensure a smoother application process for the Florida CF 831 form.
Here are key takeaways regarding the Florida CF 831 form: