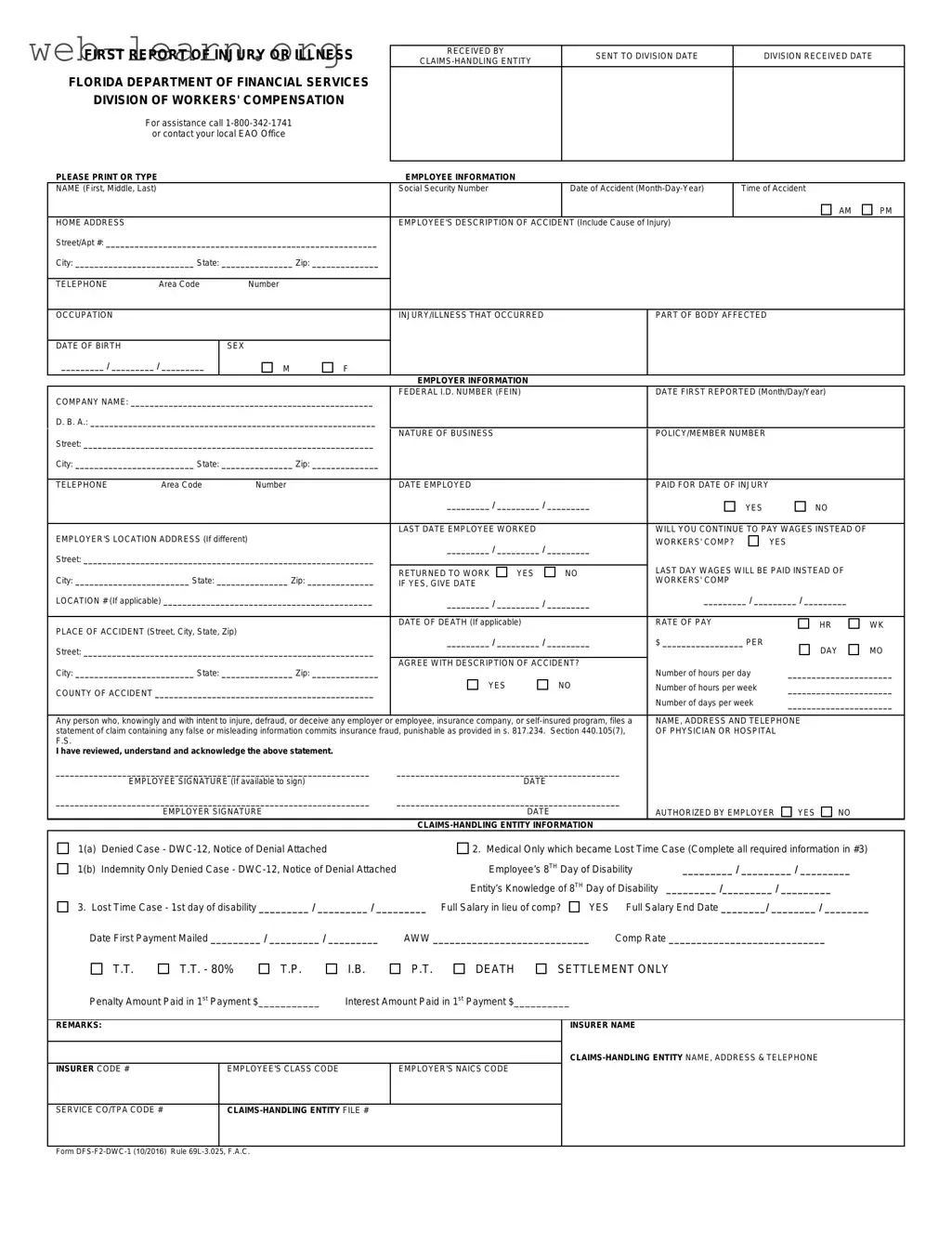
The First Report of Injury Florida form is an essential document for reporting workplace injuries or illnesses to the Division of Workers' Compensation. This form serves multiple purposes, including documenting the employee's information, the nature of the injury, and details about the employer. It requires the employee's name, Social Security number, and a description of the accident, including the time and location of the incident. Employers must also provide their company information, such as the federal ID number and the nature of their business. Importantly, the form addresses whether wages will continue to be paid instead of workers' compensation, which can significantly affect the employee's financial situation. Additionally, the form includes sections for the employer's and employee's signatures, confirming the accuracy of the information provided. Understanding how to complete this form accurately is crucial for both employees and employers, as it initiates the claims process and ensures compliance with Florida's workers' compensation laws.
| Fact Name | Description |
|---|---|
| Governing Law | The First Report of Injury form is governed by Chapter 440 of the Florida Statutes. |
| Purpose | This form is used to report workplace injuries or illnesses to the Florida Division of Workers' Compensation. |
| Submission Requirement | Employers must submit this form within seven days of being notified of an injury. |
| Employee Information | The form requires detailed employee information, including name, Social Security number, and occupation. |
| Accident Details | Employees must describe the accident, including the cause and time of the incident. |
| Employer Information | Employers must provide their name, Federal ID number, and nature of business on the form. |
| Wage Continuation | Employers must indicate if they will continue to pay wages instead of workers' compensation benefits. |
| Fraud Warning | The form includes a warning about the penalties for filing false claims, as per Section 440.105(7) of the Florida Statutes. |
| Signature Requirement | Both the employee and employer must sign the form to validate the report. |
| Contact Information | For assistance, individuals can call 1-800-342-1741 or contact their local Employee Assistance Office. |
Filling out the First Report of Injury form in Florida is an essential step in documenting workplace injuries or illnesses. After completing the form, it will need to be submitted to the appropriate claims-handling entity and the Division of Workers' Compensation. This process ensures that the injury is officially recorded and that the employee receives the necessary benefits.
What is the First Report of Injury Florida form?
The First Report of Injury form is a document used in Florida to report workplace injuries or illnesses. It is essential for employees who have sustained injuries during work to fill out this form promptly. This report helps initiate the workers' compensation process, ensuring that the injured worker receives the necessary benefits and medical care.
Who needs to fill out the form?
The injured employee is primarily responsible for completing the First Report of Injury form. However, employers are also involved in the process. They must provide specific information about the incident and their business. Both parties play a critical role in ensuring the accuracy and completeness of the report.
What information is required on the form?
The form requests various details, including:
Completing all sections accurately is crucial for a smooth claims process.
How soon must the form be submitted?
The First Report of Injury form should be submitted as soon as possible after the incident occurs. Florida law requires that employers report workplace injuries to their insurance carrier within seven days of learning about the injury. Timely submission helps ensure that the injured worker receives the benefits they need without unnecessary delays.
What happens after the form is submitted?
Once the First Report of Injury form is submitted, the claims-handling entity will review the information. They will determine whether the claim is valid and what benefits the injured worker is entitled to receive. The injured employee will be notified of the decision, and if the claim is accepted, they can begin receiving medical treatment and compensation as needed.
What if there are inaccuracies in the form?
Inaccuracies in the First Report of Injury form can lead to delays or denials of benefits. It is essential for both the employee and employer to review the information carefully before submission. If errors are discovered after submission, they should be corrected as soon as possible by notifying the claims-handling entity and providing the correct information.
When completing the First Report of Injury form in Florida, individuals often make several common mistakes that can lead to delays or complications in processing their claims. One frequent error is failing to provide complete and accurate information about the employee. This includes not only the employee's name and social security number but also the date of the accident and a detailed description of how the injury occurred. Incomplete information can hinder the claims process and may result in the claim being denied.
Another mistake involves not including the correct employer information. It is essential to ensure that the company name, federal ID number, and nature of the business are accurately reported. Omitting or misreporting these details can create confusion and complicate the verification process. Additionally, if the employer's location differs from the primary business address, this should be clearly indicated to avoid any discrepancies.
Many people also overlook the importance of documenting the date and time of the accident. This information is critical for establishing the timeline of events leading to the injury. Failure to include this data can result in questions about the legitimacy of the claim. Furthermore, it is crucial to specify whether the employee was paid for the date of injury and whether wages will continue to be paid in lieu of workers' compensation.
Another common oversight is not providing a clear description of the accident. The employee's account should detail the cause of the injury and any relevant circumstances. A vague or incomplete description can lead to misunderstandings and may affect the outcome of the claim. It is advisable to be as specific as possible to ensure that all necessary information is available for review.
People often neglect to sign the form or to have the employer's signature included. Both signatures are vital for validating the report and confirming that the information provided is accurate. Without these signatures, the form may be considered incomplete, leading to further delays in processing the claim.
Lastly, individuals sometimes fail to review the form for accuracy before submission. Simple typographical errors or omissions can have significant consequences. Taking the time to double-check all entries can prevent unnecessary complications and ensure that the claim is processed smoothly. Being thorough and meticulous when filling out the First Report of Injury form is essential for a successful claims experience.
When filing a First Report of Injury in Florida, several other forms and documents may be needed to support the claim process. Below is a list of commonly used documents that accompany the First Report of Injury form.
These documents play a vital role in the workers' compensation process. Having them prepared and submitted alongside the First Report of Injury can help ensure a smoother claims experience.
The First Report of Injury Florida form is similar to several other documents used in the context of workplace injuries and claims. Below are six documents that share similarities with the First Report of Injury form:
When filling out the First Report of Injury form in Florida, it's crucial to ensure accuracy and completeness. Here are some important dos and don’ts to keep in mind:
By following these guidelines, you can help ensure that the First Report of Injury form is filled out correctly and efficiently.
Here are 10 common misconceptions about the First Report of Injury Florida form, along with clarifications for each:
Understanding these misconceptions can help ensure that the First Report of Injury Florida form is completed accurately and submitted on time, protecting both employee rights and employer responsibilities.
Filling out the First Report of Injury form in Florida is an important step in the workers' compensation process. Here are key takeaways to keep in mind:
Following these guidelines will help ensure that the form is completed correctly and efficiently, facilitating a smoother claims process.