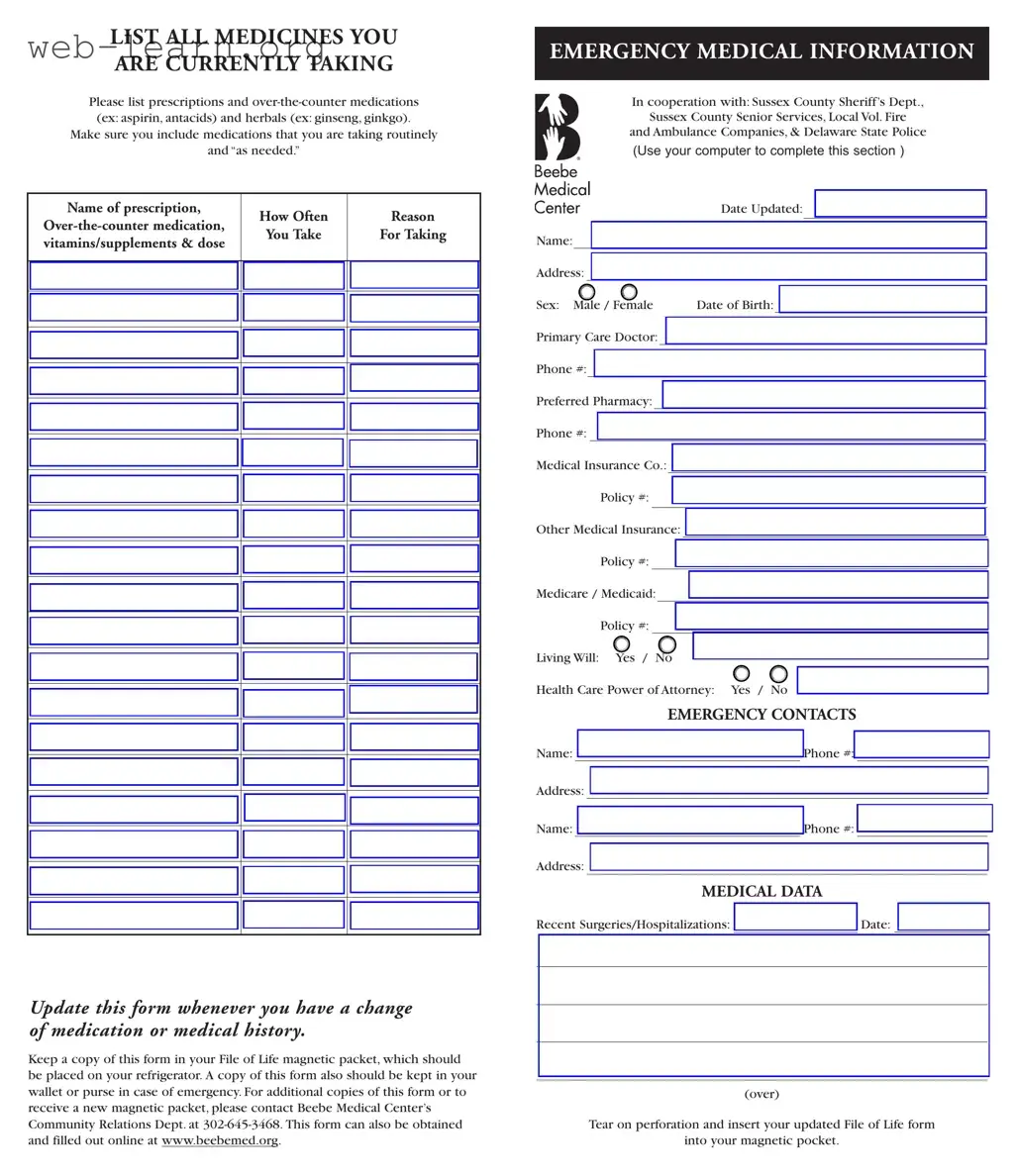
The File of Life form serves as a crucial tool for individuals to communicate essential medical information during emergencies. This form is designed to capture a comprehensive overview of a person's current medications, including both prescription and over-the-counter drugs, as well as herbal supplements. Users are encouraged to detail how often they take each medication and the reasons for their use. In addition to medication details, the form collects vital emergency medical information such as personal identification, contact information for healthcare providers, and insurance details. It also provides space for listing emergency contacts, recent surgeries, and any ongoing medical conditions. Individuals can check off various medical issues, allergies, and reactions, ensuring that first responders have a clear understanding of the patient's health status. To maintain accuracy, users are advised to update the form whenever there are changes in their medication or medical history. Keeping a copy of the File of Life form in a magnetic packet on the refrigerator and in a wallet or purse can significantly enhance safety and preparedness in emergencies. Additional copies of the form can be obtained online or through local health services, making it accessible for everyone.
| Fact Name | Description |
|---|---|
| Purpose | The File of Life form is designed to provide critical medical information to emergency responders when a person is unable to communicate their needs. |
| Contents | This form includes sections for medications, emergency contacts, medical conditions, allergies, and insurance information. |
| Medications | Users are encouraged to list all medications, including prescriptions, over-the-counter drugs, and herbal supplements, along with their dosages and purposes. |
| Emergency Contacts | It is important to include at least two emergency contacts, providing their names and phone numbers for quick access during emergencies. |
| Accessibility | The form should be kept in a magnetic packet on the refrigerator and a copy in the wallet or purse for easy access by emergency personnel. |
| Updates | Users should update the form whenever there is a change in medication or medical history to ensure accuracy. |
| Obtaining the Form | Additional copies can be requested from Beebe Medical Center’s Community Relations Department or downloaded from their website. |
| Governing Law | This form is utilized in accordance with Delaware state laws regarding medical emergency preparedness and patient information. |
| Usage in Emergencies | Emergency responders are trained to look for this form in a patient's home, making it a vital resource in critical situations. |
Filling out the File Of Life form is essential for ensuring that emergency responders have the necessary information about your medical history, medications, and emergency contacts. Follow these steps carefully to complete the form accurately.
What is the File of Life form?
The File of Life form is a vital document designed to provide emergency responders with essential medical information about an individual during a crisis. It includes details such as current medications, medical history, allergies, and emergency contacts. By having this information readily available, it can significantly improve the quality of care received in emergencies.
How should I complete the File of Life form?
To complete the File of Life form, you should list all medications you are currently taking, including prescriptions, over-the-counter drugs, and herbal supplements. For each medication, include the name, frequency of use, and the reason for taking it. Additionally, provide personal information such as your name, address, date of birth, and details about your primary care doctor and insurance. Make sure to check all relevant medical conditions and allergies.
Where should I keep the File of Life form?
It is recommended to keep the completed File of Life form in a magnetic packet on your refrigerator. This location is easily accessible for emergency responders. Additionally, you should carry a copy in your wallet or purse, ensuring that your medical information is available no matter where you are.
How often should I update the File of Life form?
Updating the File of Life form is crucial whenever there is a change in your medication, medical history, or emergency contact information. Regularly reviewing and refreshing the information ensures that it remains accurate and useful in an emergency situation.
How can I obtain additional copies of the File of Life form?
If you need additional copies of the File of Life form or a new magnetic packet, you can contact Beebe Medical Center’s Community Relations Department at 302-645-3468. Alternatively, the form can also be accessed and filled out online at www.beebemed.org.
Filling out the File Of Life form is crucial for ensuring your health information is accessible in emergencies. However, many individuals make common mistakes that can compromise the effectiveness of this important document. One prevalent error is failing to list all medications. It is essential to include every prescription, over-the-counter medication, and herbal supplement you take. Omitting even one can lead to dangerous interactions or inadequate treatment during a medical emergency.
Another mistake involves not updating the form regularly. Medical conditions and medications can change frequently. Neglecting to revise your File Of Life form after any significant health change can result in outdated information being provided to emergency responders. This oversight can delay appropriate care and may even worsen your condition.
People often overlook the importance of including emergency contacts. Providing accurate names and phone numbers for family members or friends who can be reached in an emergency is vital. In some cases, individuals may list contacts who are unavailable or unreachable, which can hinder timely communication during critical moments.
Additionally, many individuals do not specify the dosage of their medications. Simply naming a medication without detailing how much you take can lead to confusion. Emergency personnel need precise information to administer the correct treatment, especially if they need to provide medications in a critical situation.
Some individuals mistakenly assume that their primary care doctor’s information is unnecessary. It is vital to include your doctor’s name and phone number on the form. This information allows emergency responders to quickly reach out for additional medical history or guidance, ensuring that you receive the best possible care.
Lastly, failing to indicate allergies and reactions can have severe consequences. If you have allergies to specific medications or substances, clearly stating them on the form is imperative. Emergency responders must know this information to avoid administering anything that could trigger a dangerous reaction.
The File Of Life form is a crucial document for ensuring that emergency responders have immediate access to your medical information. Alongside this form, there are several other important documents that can provide additional context and details about your health. Here’s a brief overview of four commonly used forms that complement the File Of Life form.
By keeping these documents updated and accessible, you can ensure that your medical information is clear and available when it matters most. It’s always a good idea to review these forms regularly and make any necessary changes to reflect your current health status.
The File of Life form serves as a vital tool for individuals to communicate their medical information effectively in emergencies. Several other documents share similarities with the File of Life form in terms of purpose and content. Below is a list of seven documents that are comparable:
When filling out the File of Life form, it is important to ensure accuracy and clarity. Here are some guidelines to follow:
Following these guidelines will help ensure that your File of Life form is both effective and useful in an emergency situation.
Understanding the File of Life form is essential for ensuring that emergency responders have the necessary information to provide appropriate care. However, several misconceptions can lead to confusion about its purpose and use. Here are ten common misconceptions:
Here are six key takeaways about filling out and using the File Of Life form: