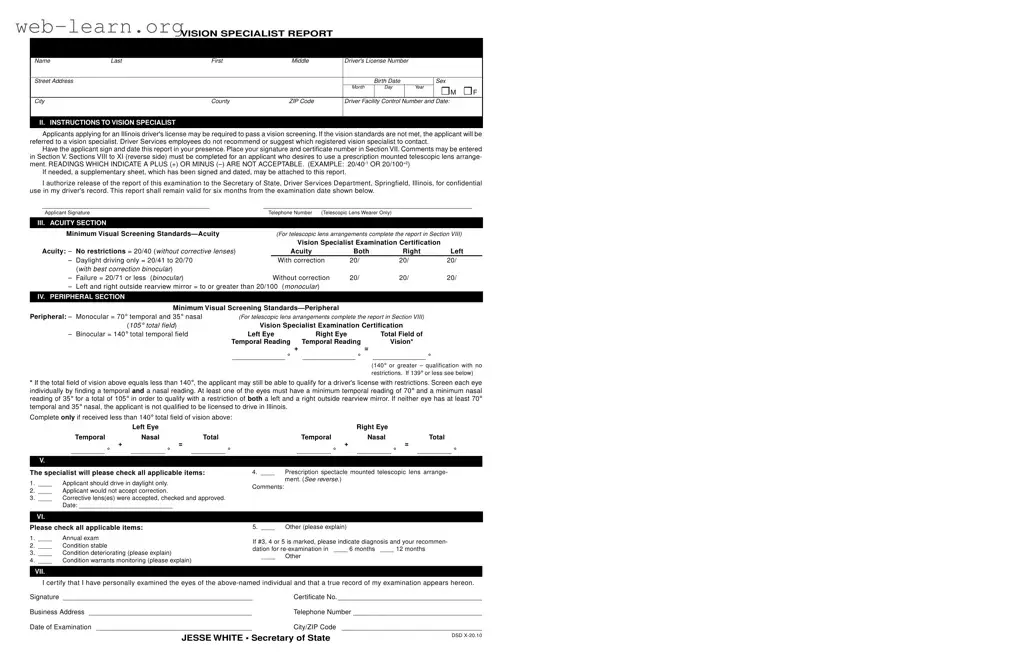
The DMV Vision Test Illinois form is an essential document for individuals applying for a driver's license in the state of Illinois, particularly for those who may need to meet specific vision standards. This form collects important applicant information, including the individual’s name, address, and driver’s license number, alongside details about their vision specialist. The process begins with a vision screening, and if the applicant does not meet the required standards, they are referred to a vision specialist for further evaluation. The vision specialist must complete various sections of the form, documenting the applicant's visual acuity and peripheral vision. For those who require prescription telescopic lenses, additional sections must be filled out to ensure compliance with specific visual requirements. Importantly, the form outlines that readings indicating a plus or minus are not acceptable, emphasizing the need for precise measurement. The applicant must also authorize the release of their examination results to the Secretary of State, ensuring that their driving record reflects their vision status. This form remains valid for six months from the examination date, making timely submission crucial for those looking to obtain or renew their driver's license.

| Fact Name | Description |
|---|---|
| Applicant Information | The form collects essential details such as the applicant's name, address, birth date, and driver's license number. |
| Vision Screening Requirement | Applicants may need to pass a vision screening. If they do not meet the standards, they will be referred to a vision specialist. |
| Minimum Visual Standards | To qualify, applicants must achieve a minimum acuity of 20/40 without corrective lenses or 20/70 with correction. |
| Peripheral Vision Standards | Applicants must have a minimum temporal field of 70° and a nasal field of 35° for a total of 105° to qualify for a driver's license. |
| Governing Law | This form is governed by the Illinois Vehicle Code, specifically related to driver licensing and vision requirements. |
Completing the DMV Vision Test form in Illinois is an essential step for individuals applying for a driver's license, especially if a vision screening is required. This form helps document the results of the vision examination and provides necessary information to the Secretary of State's office. Follow the steps below to accurately fill out the form.
What is the purpose of the DMV Vision Test Illinois form?
The DMV Vision Test Illinois form is utilized to assess the visual acuity and peripheral vision of individuals applying for a driver's license in Illinois. If an applicant does not meet the minimum vision standards during the initial screening, they are referred to a vision specialist. This form serves as a record of that examination and includes critical information about the applicant's vision capabilities.
Who needs to complete the vision test?
Individuals applying for a driver's license in Illinois may be required to undergo a vision screening. If they do not meet the necessary vision standards, they must have the vision specialist complete the DMV Vision Test form. This requirement applies to both new applicants and those renewing their licenses if their vision has changed.
What are the minimum visual screening standards?
The minimum visual screening standards vary based on whether the applicant has corrective lenses. For those without corrective lenses, a visual acuity of 20/40 is required for unrestricted driving. If an applicant's vision is between 20/41 and 20/70, they may be limited to daylight driving only. A visual acuity of 20/71 or less indicates a failure to meet the necessary standards. Additionally, peripheral vision requirements mandate a minimum of 70° temporal and 35° nasal vision for monocular applicants.
What should a vision specialist include in their report?
The vision specialist must complete several sections of the form, including the acuity and peripheral sections. They should also provide their signature and certificate number to certify the examination. Comments regarding the applicant's vision condition and recommendations for re-examination should be included if necessary. It is important for the specialist to indicate whether the applicant's condition is stable or deteriorating.
How long is the vision test report valid?
The DMV Vision Test report remains valid for six months from the date of the examination. This time frame allows applicants to submit their results in a timely manner when applying for or renewing their driver's license.
What if an applicant requires a telescopic lens arrangement?
Applicants who qualify to drive with a prescription spectacle mounted telescopic lens arrangement must have specific visual standards met, including a central acuity of 20/40 or better through the telescopic lens. They will be restricted to driving during daylight hours only. The vision specialist must complete additional sections of the form specifically addressing the requirements for telescopic lens wearers.
Completing the DMV Vision Test form in Illinois can be straightforward, but many applicants make common mistakes that can delay their application process. One frequent error is not signing the form in the presence of the vision specialist. The applicant must sign and date the report while the specialist is present. If this step is overlooked, it could lead to rejection of the form.
Another mistake involves incorrect completion of the acuity section. Applicants often fail to provide the correct visual acuity readings. For instance, using a plus (+) or minus (–) sign in the readings is not acceptable. This can lead to confusion and the need for a resubmission. Ensure that the readings are clearly noted without any symbols.
Additionally, some applicants neglect to complete the peripheral vision section properly. Each eye must be assessed individually, and the total field of vision must be calculated accurately. If the readings do not meet the minimum requirements, the applicant may not qualify for a driver's license. It’s essential to double-check these measurements before submission.
Another common oversight is failing to include necessary comments in Section V. If there are any specific conditions or observations that need to be noted, they should be included. Leaving this section blank could result in additional questions or complications later in the process.
Moreover, applicants sometimes forget to check all applicable items in the specialist's certification sections. It’s crucial to mark all relevant conditions, such as whether the applicant should drive only during daylight hours. Missing these details can lead to misunderstandings regarding driving privileges.
Finally, not providing a valid contact number can be a significant mistake. This information is important for any follow-up or clarification needed by the DMV. Ensure that all contact details are accurate and up-to-date to avoid unnecessary delays.
When preparing to take the DMV Vision Test in Illinois, several other forms and documents may be required or beneficial. These documents can help ensure a smooth process and provide the necessary information for your application. Below is a list of these forms, along with a brief description of each.
Having these documents ready can streamline the process of applying for a driver's license in Illinois. Each form plays a vital role in ensuring that applicants meet the necessary requirements to drive safely and legally.
The DMV Vision Test Illinois form is essential for applicants seeking a driver's license in Illinois. Several other documents serve similar purposes in assessing an individual's vision capabilities for driving. Here are five documents that share similarities with the DMV Vision Test Illinois form:
When filling out the DMV Vision Test form in Illinois, there are important guidelines to follow. Here’s a list of things you should and shouldn’t do:
By following these guidelines, you can ensure a smoother experience while completing the DMV Vision Test form.
There are several misconceptions surrounding the DMV Vision Test in Illinois that can create confusion for applicants. Here are seven of the most common misunderstandings:
Understanding these misconceptions can help applicants prepare more effectively for the DMV Vision Test in Illinois. Being informed ensures that you meet all necessary requirements and can proceed smoothly through the licensing process.
When applying for an Illinois driver's license, a vision screening is often required. If the applicant does not meet the vision standards, they must see a vision specialist.
It’s essential to have the applicant sign and date the vision test report in the presence of the vision specialist. This ensures the authenticity of the document.
Readings that include plus (+) or minus (–) signs are not acceptable. For example, formats like 20/40-1 or 20/100+2 will not be recognized.
The report remains valid for six months from the examination date. Make sure to submit it within this timeframe to avoid any issues.
If the applicant uses a prescription telescopic lens, additional sections of the form must be completed. This includes specific acuity and peripheral vision standards.