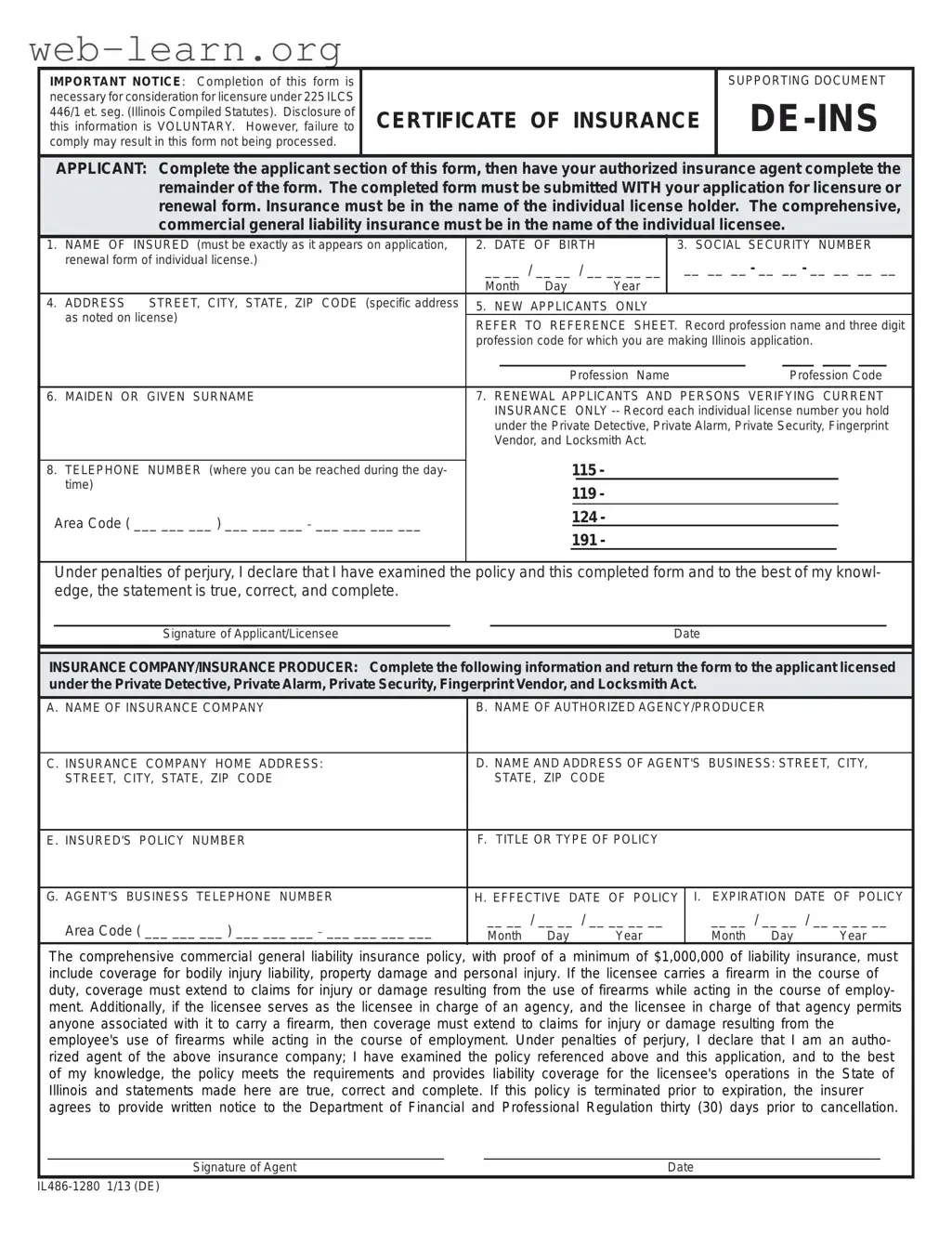
The De Ins Illinois form plays a crucial role in the licensing process for various professions in the state, including private detectives and security personnel. It serves as a supporting document that must be completed alongside the application for licensure or renewal. The form requires applicants to provide essential information such as their name, date of birth, and social security number. Additionally, applicants must indicate their profession and provide the corresponding profession code. Importantly, the form also necessitates the involvement of an authorized insurance agent, who will fill out the insurance details, ensuring that the applicant has the required comprehensive commercial general liability insurance. This insurance must cover a minimum of $1,000,000 for bodily injury, property damage, and personal injury, extending to claims related to the use of firearms if applicable. Failure to complete this form accurately may lead to delays or denial in the licensing process, emphasizing the need for careful attention to detail.
| Fact Name | Fact Description |
|---|---|
| Governing Law | This form is governed by 225 ILCS 446/1 et seq. of the Illinois Compiled Statutes. |
| Purpose | Completion of the form is necessary for consideration for licensure under the specified statutes. |
| Voluntary Disclosure | Disclosure of information on the form is voluntary; however, failure to comply may lead to non-processing. |
| Insurance Requirements | The insurance must be comprehensive, commercial general liability with a minimum coverage of $1,000,000. |
| Submission Process | The completed form must be submitted with the application for licensure or renewal. |
| Agent's Responsibilities | The authorized insurance agent must complete the remainder of the form after the applicant fills out their section. |
Filling out the De Ins Illinois form is an essential step for those seeking licensure in Illinois. Ensure that all information is accurate and complete to avoid processing delays. Follow the steps below to successfully complete the form.
Next, the insurance company or authorized agent will need to complete their section of the form. This includes providing details about the insurance policy and confirming that it meets the necessary requirements. After both sections are filled out, submit the completed form with your application for licensure or renewal.
What is the purpose of the De Ins Illinois form?
The De Ins Illinois form is a supporting document required for individuals seeking licensure under the Illinois Compiled Statutes. It is necessary to provide proof of comprehensive commercial general liability insurance. This insurance must cover the individual license holder and ensure that they are protected against various liabilities while performing their professional duties.
Who needs to complete the De Ins Illinois form?
Both new applicants and renewal applicants must complete this form. New applicants need to fill out their personal information and have their authorized insurance agent complete the rest. Renewal applicants should also provide their current insurance details. It is crucial that the completed form is submitted along with the application for licensure or renewal.
What information is required on the form?
The form requires several pieces of information, including:
Additionally, the insurance company and agent must provide their details, including the policy number, type of policy, effective dates, and coverage amounts.
What are the insurance requirements for the De Ins Illinois form?
The insurance policy must be a comprehensive commercial general liability insurance with a minimum coverage of $1,000,000. It should cover bodily injury liability, property damage, and personal injury. If the licensee carries a firearm during their work, the policy must also cover claims related to firearm use. This coverage extends to any employees authorized to carry firearms under the licensee's agency.
Filling out the De Ins Illinois form can be a straightforward process, but many applicants make common mistakes that can delay their licensure. One frequent error is failing to ensure that the name of the insured matches exactly with the name on the application. This inconsistency can lead to processing issues, as the state requires precise information for verification.
Another common mistake involves neglecting to provide a complete and accurate date of birth. It's essential to double-check this information, as any discrepancies may raise red flags during the review process. Similarly, applicants often overlook the requirement to include their Social Security number. This detail is crucial for identification and verification purposes, and omitting it can result in a rejection of the form.
Applicants should also be cautious when filling out their address. A specific address is required, and any errors in the street name, city, or zip code can lead to complications. Moreover, new applicants frequently forget to reference the profession name and three-digit profession code, which are necessary for the application. This oversight can cause unnecessary delays in processing.
Another mistake that can occur is not providing a valid telephone number where the applicant can be reached during the day. This information is important for any follow-up questions or clarifications. Lastly, applicants sometimes neglect to have their authorized insurance agent complete the necessary sections of the form. This step is vital, as the agent’s information and signature validate the insurance coverage, which is a key component of the application.
By avoiding these common pitfalls, applicants can ensure a smoother application process. Paying attention to detail and double-checking all entries will save time and help secure the necessary licensure in Illinois.
When applying for licensure in Illinois, particularly in the fields governed by the Private Detective, Private Alarm, Private Security, Fingerprint Vendor, and Locksmith Act, several forms and documents accompany the De Ins Illinois form. Each of these documents plays a crucial role in ensuring that your application is complete and meets the necessary legal requirements. Below is a list of these important forms and documents.
Submitting the correct forms and documents alongside the De Ins Illinois form is vital for a smooth application process. Each document serves a specific purpose and helps to verify that the applicant meets the necessary standards for licensure. Ensuring that all paperwork is complete and accurate will significantly enhance the chances of a successful application.
The De Ins Illinois form is essential for those seeking licensure in specific professions. It is similar to several other documents that also serve as proof of compliance and insurance coverage. Below is a list of documents that share similarities with the De Ins Illinois form:
Each of these documents plays a vital role in ensuring that professionals meet the necessary standards for licensure and compliance within their respective fields.
When filling out the De Ins Illinois form, it is important to approach the task with care. Here are some essential dos and don’ts to keep in mind:
By following these guidelines, you can help ensure that your application is processed smoothly and efficiently.
This form is mandatory for consideration of licensure. Without it, your application may not be processed.
Insurance coverage is required. It must be in the name of the individual license holder.
The comprehensive general liability insurance must be in the name of the individual licensee, not a business entity.
The applicant must complete their section, but an authorized insurance agent must fill out the remainder.
Details like the policy number, effective dates, and coverage type are essential and must be included.
The completed form must accompany your application for licensure or renewal. Timing matters.
A minimum of $1,000,000 liability coverage is required. This is non-negotiable.
Coverage must include bodily injury, property damage, and personal injury. All aspects are crucial.
If the policy is terminated before expiration, the insurer must provide written notice to the Department 30 days prior to cancellation.
Filling out the De Ins Illinois form can seem daunting, but understanding its key components will make the process smoother. Here are some essential takeaways to keep in mind:
By keeping these points in mind, you can ensure that your De Ins Illinois form is filled out correctly and submitted on time, paving the way for a smoother licensure process.