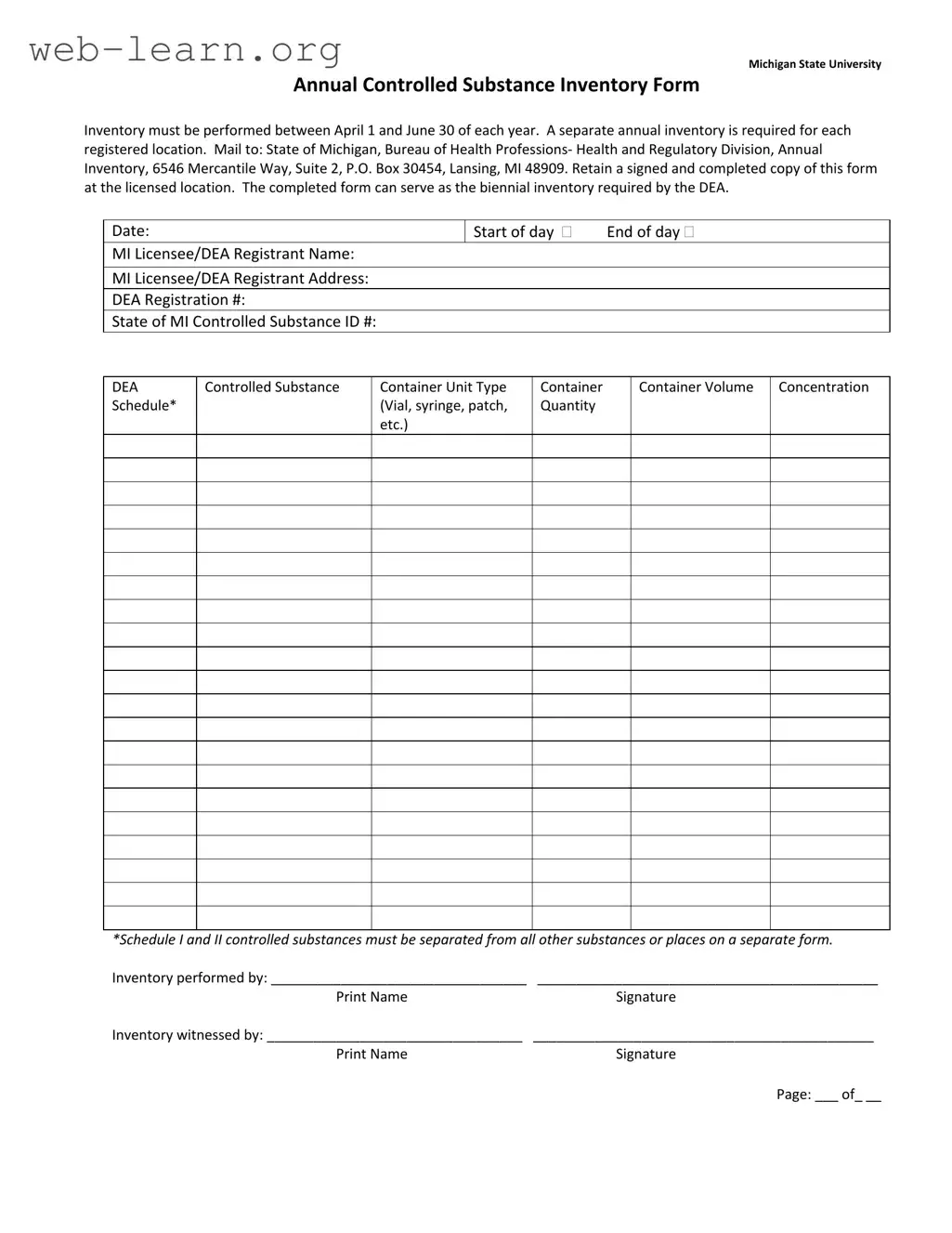
The Control Substance Inventory Michigan form is a crucial document for any facility that handles controlled substances in the state. Each year, an inventory must be conducted between April 1 and June 30, ensuring compliance with state regulations. This form requires a separate inventory for each registered location, which helps maintain accurate records and accountability. Once completed, the form should be mailed to the Bureau of Health Professions in Lansing. It is important to keep a signed copy at the licensed location for your records. Notably, this form can also fulfill the biennial inventory requirement set by the DEA, streamlining the compliance process. Key information collected includes the date of inventory, the name and address of the DEA registrant, and specific details about the controlled substances, such as their schedule classification and container types. For substances classified as Schedule I and II, special attention is required, as they must be documented separately. Additionally, the form mandates signatures from both the person conducting the inventory and a witness, further ensuring the integrity of the process.
| Fact Name | Details |
|---|---|
| Inventory Period | The inventory must be conducted between April 1 and June 30 each year. |
| Location Requirement | A separate annual inventory is necessary for each registered location. |
| Mailing Address | Send the completed form to the Bureau of Health Professions at the specified Lansing address. |
| Retention Policy | Keep a signed and completed copy of the form at the licensed location for records. |
| DEA Compliance | The completed form can fulfill the biennial inventory requirement set by the DEA. |
Completing the Control Substance Inventory Michigan form is a crucial step for maintaining compliance with state regulations. This process involves gathering specific information about controlled substances at your registered location. After filling out the form, it will need to be mailed to the appropriate state office, and a signed copy should be kept on file for your records.
What is the purpose of the Controlled Substance Inventory Michigan form?
The Controlled Substance Inventory Michigan form is used to document the annual inventory of controlled substances held by licensed facilities in Michigan. This inventory must be conducted between April 1 and June 30 each year. It ensures compliance with state regulations and helps maintain accurate records of controlled substances.
Who is required to complete this inventory?
Every facility that holds a license to manage controlled substances in Michigan must complete this inventory. Each registered location must have a separate annual inventory form. This requirement applies to various entities, including hospitals, pharmacies, and research institutions.
How should the completed form be submitted?
Once the inventory is completed, the form should be mailed to the following address:
It is important to retain a signed and completed copy of this form at the licensed location for record-keeping purposes.
What specific information is required on the form?
The form requires detailed information including:
It is crucial that Schedule I and II controlled substances are recorded separately or on a different form.
Can this form be used for DEA biennial inventory requirements?
Yes, the completed Michigan Controlled Substance Inventory form can serve as the biennial inventory required by the DEA. By maintaining this documentation, facilities can ensure compliance with both state and federal regulations regarding controlled substances.
Filling out the Control Substance Inventory Michigan form requires careful attention to detail. One common mistake individuals make is failing to perform the inventory within the designated time frame. The form specifies that the inventory must occur between April 1 and June 30 each year. Missing this window can lead to compliance issues.
Another frequent error involves neglecting to submit a separate inventory for each registered location. Each facility must have its own completed form, as combining inventories can create confusion and may not meet regulatory requirements. This oversight can result in significant penalties.
People often overlook the requirement to mail the completed form to the correct address. The form must be sent to the Bureau of Health Professions at the specified Lansing address. Sending it to an incorrect location can delay processing and compliance verification.
Inaccurate information about the registrant can also lead to complications. Individuals frequently forget to include their DEA Registration number or provide incorrect details for the MI Licensee/DEA Registrant Name and Address. Such inaccuracies can hinder the processing of the inventory.
Another mistake arises when individuals fail to separate Schedule I and II controlled substances from other substances. These substances must be listed on a separate form, as indicated in the instructions. Failing to do so can lead to serious compliance issues and potential legal ramifications.
Moreover, some people do not retain a signed copy of the completed form at the licensed location. This step is crucial for record-keeping and may be required during inspections or audits. Without a retained copy, proving compliance can become problematic.
Errors in detailing the controlled substances can also occur. Individuals may incorrectly list the container type, quantity, or volume. Each of these details is essential for accurate inventory tracking and compliance with state and federal regulations.
Lastly, failing to have the inventory witnessed by another individual can be a significant oversight. The form requires signatures from both the person performing the inventory and a witness. Not securing a witness can invalidate the inventory and lead to further complications.
When managing controlled substances, various forms and documents are essential to ensure compliance with state and federal regulations. Each document serves a specific purpose in the inventory and management process, helping to maintain accountability and safety. Here are some commonly used forms alongside the Control Substance Inventory Michigan form:
Understanding these forms and their purposes is crucial for anyone involved in the management of controlled substances. Proper documentation not only ensures compliance with legal requirements but also promotes safety and accountability in handling these sensitive materials.
The Control Substance Inventory Michigan form shares similarities with several other important documents in the realm of controlled substances. Here are four of them:
When filling out the Control Substance Inventory Michigan form, it’s essential to follow specific guidelines to ensure accuracy and compliance. Here are some important dos and don'ts to consider:
This is incorrect. The inventory must be conducted specifically between April 1 and June 30 each year.
Each registered location requires a separate annual inventory. This ensures accurate tracking of controlled substances at each site.
It is essential to mail the completed form to the Bureau of Health Professions at the specified Lansing address to comply with regulations.
It is important to keep a signed and completed copy of the inventory at the licensed location for your records.
While Schedule I and II substances have specific requirements, the form applies to all controlled substances listed in the inventory.
Having a witness sign the inventory is a crucial step in the process. It adds an extra layer of accountability and verification.
The completed inventory form can also fulfill the biennial inventory requirement set by the DEA, making it a valuable document.
Accurate details regarding container types, quantities, and volumes are necessary for compliance and tracking purposes.
When filling out and using the Controlled Substance Inventory Michigan form, keep these key takeaways in mind:
By adhering to these guidelines, the inventory process will be more efficient and compliant with state and federal regulations.