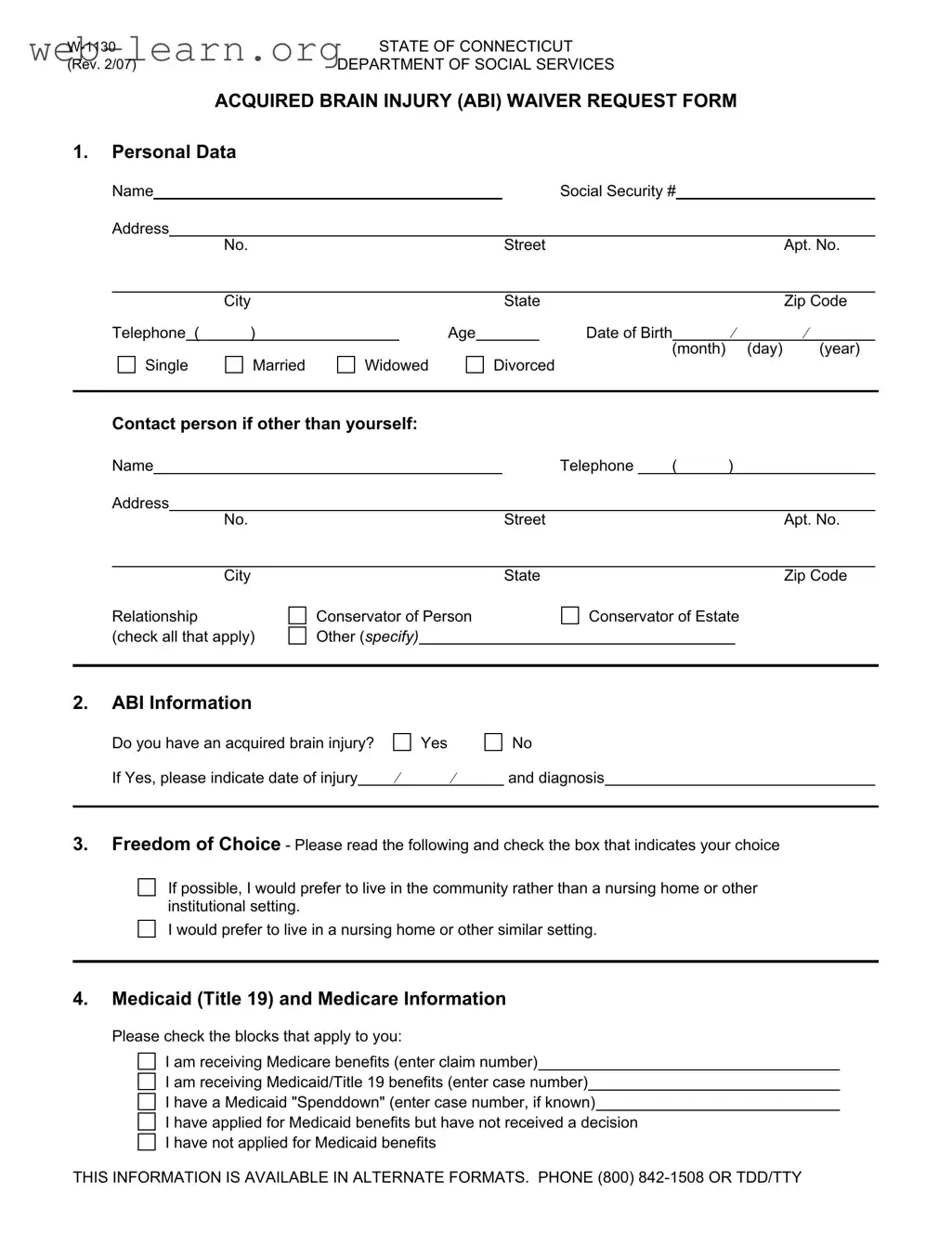
The Connecticut W 1130 form is a vital document for individuals seeking assistance through the Acquired Brain Injury (ABI) Waiver program. This form serves as a request for support from the Department of Social Services, specifically designed for those who have experienced an acquired brain injury. It collects essential personal information, such as the applicant's name, address, and contact details, as well as critical data regarding their injury and medical history. Additionally, the form addresses the applicant's living preferences, allowing individuals to express their desire to remain in the community rather than transition to a nursing home or institutional setting. It also includes sections to gather information about Medicaid and Medicare benefits, ensuring that applicants receive the appropriate financial support. The form further requests details about the applicant's monthly income and total assets, which are necessary for determining eligibility for assistance. Overall, the Connecticut W 1130 form is a comprehensive tool that facilitates access to necessary services for individuals affected by acquired brain injuries, promoting their well-being and independence.

| Fact Name | Description |
|---|---|
| Form Purpose | The W-1130 form is a request for the Acquired Brain Injury (ABI) Waiver in Connecticut. |
| Governing Law | This form is governed by the Connecticut General Statutes, specifically Section 17b-260. |
| Eligibility Requirement | Applicants must have a documented acquired brain injury to qualify for the waiver. |
| Community Preference | The form allows applicants to express a preference for living in the community versus an institutional setting. |
| Medicaid and Medicare | Applicants must provide information regarding their Medicaid and Medicare benefits, if applicable. |
| Submission Address | The completed form should be sent to the Department of Social Services at 25 Sigourney Street, Hartford, CT 06106-5033. |
Completing the Connecticut W-1130 form is a straightforward process. After gathering the necessary information, you will provide personal details, information about your brain injury, and financial data. Ensure that you have all relevant documents at hand to make filling out the form easier.
The Connecticut W 1130 form is a request form for the Acquired Brain Injury (ABI) Waiver. It is designed for individuals who have suffered an acquired brain injury and are seeking assistance to live in the community rather than in institutional settings. This form collects personal data, ABI information, Medicaid and Medicare status, and financial data to assess eligibility for the waiver program.
The form should be completed by individuals who have an acquired brain injury. If the individual is unable to complete the form themselves, a conservator or other representative may fill it out on their behalf. It is important to ensure that all information is accurate and complete to facilitate the review process.
The W 1130 form requires several pieces of information:
Once the form is completed, it should be sent to the Department of Social Services at:
Department of Social Services
25 Sigourney Street
Hartford, CT 06106-5033
Attention: Social Work Services, 10th Floor.
If you have questions or need assistance while filling out the form, you can contact the Department of Social Services. They can provide guidance and answer any specific questions you may have. Additionally, the information is available in alternate formats for those who require it. You can reach them at (800) 842-1508 or TDD/TTY at (800) 842-4524.
After submission, the Department of Social Services will review the application to determine eligibility for the ABI Waiver. You may be contacted for additional information or clarification during this process. It’s important to keep track of any correspondence and respond promptly to ensure a smooth review of your request.
Filling out the Connecticut W-1130 form can seem straightforward, but there are common mistakes that applicants often make. Understanding these pitfalls can help ensure a smoother application process. One frequent error is neglecting to provide complete personal data. Missing information, such as the Social Security number or date of birth, can delay processing. Always double-check that every required field is filled out accurately.
Another common mistake is failing to specify the acquired brain injury (ABI) details. Applicants should indicate the date of injury and diagnosis clearly. Omitting this information may lead to misunderstandings about eligibility. It’s crucial to be thorough and precise when describing the ABI to avoid complications later in the process.
Many applicants also overlook the section regarding freedom of choice. This part of the form allows individuals to express their living preferences. Some may forget to check a box, which can result in confusion about their wishes. It’s important to take a moment to consider where one would prefer to live and indicate that choice clearly.
When it comes to Medicaid and Medicare information, applicants sometimes make the mistake of providing incomplete or inaccurate details. For instance, if receiving Medicare benefits, it’s essential to enter the correct claim number. Similarly, if applying for Medicaid, ensuring that the case number is accurate is vital. Errors in this section can lead to delays or denials of benefits.
Financial data is another area where mistakes commonly occur. Applicants may miscalculate their total monthly income or assets. This can lead to discrepancies that affect eligibility. It’s wise to gather all relevant financial documents before filling out this section to ensure accuracy.
Lastly, forgetting to sign the form is a frequent oversight. Both the applicant and any conservator or representative must provide their signatures. Without these, the application cannot be processed. Before submitting, it’s beneficial to review the entire form to confirm that all signatures are present and correct.
The Connecticut W-1130 form is used to request services under the Acquired Brain Injury (ABI) Waiver program. It collects personal, financial, and medical information about the applicant. Several other forms and documents are often required to support the application process. Below is a list of these related documents.
These documents play a critical role in the application process for the ABI Waiver program in Connecticut. Proper completion and submission of these forms can help ensure that individuals receive the support and services they need.
The Connecticut W 1130 form is designed for individuals seeking assistance under the Acquired Brain Injury (ABI) Waiver program. Several other documents serve similar purposes in terms of collecting personal and financial information for various assistance programs. Below are six documents that share similarities with the W 1130 form:
Each of these forms shares a common goal: to assess eligibility for various forms of assistance by collecting vital information from applicants. Understanding these similarities can help individuals navigate the process of applying for the support they need.
When filling out the Connecticut W-1130 form, there are several important dos and don'ts to keep in mind. Following these guidelines can help ensure that your application is processed smoothly.
By adhering to these guidelines, you can help facilitate a smoother experience with the Connecticut W-1130 form. Make sure to review your answers before submitting to avoid any delays in processing.
Misconceptions can lead to confusion, especially when it comes to important forms like the Connecticut W 1130. Here are some common misunderstandings about this form that you should be aware of:
Understanding these misconceptions is vital for anyone considering the W 1130 form. Taking the time to clarify these points can help streamline the application process and improve the chances of receiving the necessary support.
The Connecticut W 1130 form is essential for individuals seeking assistance under the Acquired Brain Injury (ABI) Waiver program. Proper completion of this form is crucial for eligibility determination. Here are key takeaways regarding its use:
Completing the W 1130 form accurately and promptly is vital for securing necessary services. Be diligent in gathering all required information before submission to avoid delays.