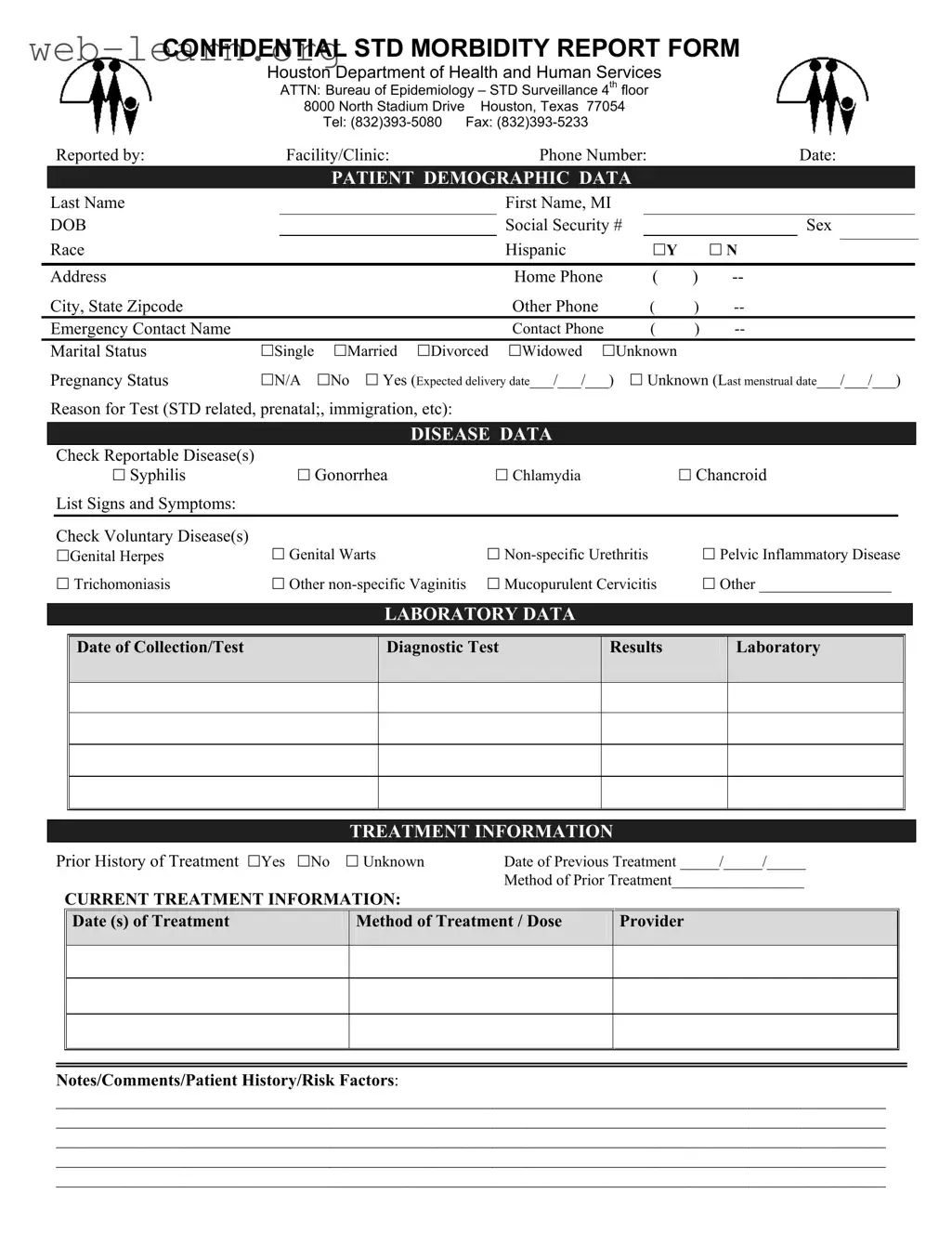
The Connecticut UC 2 form plays a crucial role in the reporting and tracking of sexually transmitted diseases (STDs) within the state. Designed to collect essential patient demographic data, the form includes sections for personal information such as name, date of birth, and contact details, ensuring that health officials can accurately identify and follow up with individuals. Additionally, it requires information about the patient's marital status and pregnancy status, which can be important for public health monitoring. The form also encompasses disease data, where healthcare providers can check off reportable diseases like syphilis, gonorrhea, and chlamydia, as well as voluntary diseases such as genital herpes and pelvic inflammatory disease. Laboratory data is captured, including the date of sample collection and diagnostic test results, which are vital for understanding the spread of STDs. Treatment information is another key aspect, detailing prior and current treatment methods, dates, and any relevant patient history. By providing a comprehensive overview of these elements, the UC 2 form aids in the effective management and prevention of STDs, ultimately contributing to better public health outcomes in Connecticut.
| Fact Name | Description |
|---|---|
| Form Purpose | The Connecticut UC 2 form is designed to collect confidential morbidity data related to sexually transmitted diseases (STDs) for public health monitoring. |
| Governing Law | This form is governed by the Connecticut General Statutes, particularly sections related to public health and disease reporting. |
| Confidentiality | All information provided on the UC 2 form is confidential and is used solely for health surveillance purposes. |
| Data Required | Required data includes patient demographics, disease data, laboratory results, and treatment information. |
| Submission Guidelines | The completed form must be submitted to the appropriate health department office as specified in the instructions. |
| Reporting Timeline | Health care providers are required to report cases of STDs within a specific timeframe as mandated by state law. |
After gathering the necessary information, you can begin filling out the Connecticut UC 2 form. Be sure to provide accurate details to ensure proper processing. Follow these steps carefully.
Once you have completed the form, review all entries for accuracy. After that, submit the form to the appropriate department as indicated at the top. Make sure to keep a copy for your records.
What is the Connecticut UC 2 form?
The Connecticut UC 2 form is a confidential morbidity report used for reporting sexually transmitted diseases (STDs) to the appropriate health authorities. It is essential for tracking and managing public health concerns related to STDs. The form collects demographic data, disease data, laboratory information, and treatment history to ensure comprehensive reporting.
Who is required to fill out the UC 2 form?
Healthcare providers, including doctors, clinics, and hospitals, are responsible for completing the UC 2 form when they diagnose a patient with a reportable STD. This requirement helps health officials monitor the incidence of STDs and implement necessary public health interventions.
What information is required on the UC 2 form?
The form requires various details, including:
Completing all sections accurately is crucial for effective disease surveillance and response.
How is the information on the UC 2 form used?
The data collected through the UC 2 form is utilized by public health authorities to monitor STD trends, identify outbreaks, and develop targeted prevention strategies. This information is vital for improving community health outcomes and ensuring that resources are allocated effectively.
Is the information on the UC 2 form confidential?
Yes, the information submitted on the UC 2 form is confidential. It is protected under privacy laws, ensuring that patient identities remain secure. Only authorized personnel within public health departments have access to this data for epidemiological purposes.
Where should the completed UC 2 form be sent?
The completed UC 2 form should be sent to the Houston Department of Health and Human Services, specifically to the Bureau of Epidemiology – STD Surveillance. The mailing address is:
8000 North Stadium Drive, 4th Floor
Houston, Texas 77054
Additionally, forms can be submitted via fax at (832) 393-5233.
Filling out the Connecticut UC 2 form can be a straightforward process, but there are common mistakes that can lead to delays or issues in processing. One frequent error is providing incomplete patient demographic data. Missing information such as the last name, date of birth, or social security number can cause significant setbacks. It is crucial to double-check that all fields are filled out accurately before submission.
Another mistake often made is failing to accurately report the reason for the test. This section is vital for understanding the context of the patient's visit. If the reason is unclear or not specified, it can lead to confusion for healthcare providers. Clear communication about the reason for testing is essential to ensure appropriate follow-up and treatment.
Many individuals overlook the importance of checking the reportable diseases correctly. Not marking the relevant diseases can result in incomplete data collection, which affects public health monitoring. Ensure that all applicable diseases are checked off. If unsure, it is better to consult with a healthcare provider for clarification.
In the treatment information section, people sometimes provide vague or incomplete details about prior treatments. This can hinder effective treatment planning. Specific dates and methods of previous treatments should be recorded clearly. Providing comprehensive treatment history helps healthcare professionals make informed decisions.
Lastly, neglecting to include notes or comments about patient history or risk factors can be detrimental. This section allows for additional context that may be relevant to the patient's care. Detailed notes can significantly enhance the understanding of the patient's situation, leading to better health outcomes. Always take the time to provide thorough information in this area.
When submitting the Connecticut UC 2 form, there are several other forms and documents that may be necessary to ensure comprehensive reporting and compliance with health regulations. Each of these documents serves a specific purpose and helps facilitate effective communication between healthcare providers and public health authorities.
Utilizing these additional forms alongside the Connecticut UC 2 form can enhance the accuracy of reporting and improve patient care outcomes. Each document plays a vital role in the overall process, ensuring that patient information is managed effectively and responsibly.
When filling out the Connecticut UC 2 form, there are several important dos and don'ts to keep in mind. Following these guidelines can help ensure that the form is completed accurately and efficiently.
Understanding the Connecticut UC 2 form can be challenging, and misconceptions often arise. Here are ten common misunderstandings about this form, along with clarifications to help you navigate the process more effectively.
While the UC 2 form includes sections for STDs, it can also be used for other health-related reporting, such as prenatal or immigration-related tests.
The information collected on the UC 2 form is confidential and is protected by privacy laws. It is only accessible to authorized personnel.
The form allows for the reporting of multiple diseases. You can check all applicable reportable and voluntary diseases in the designated sections.
While it is important to provide as much information as possible, incomplete forms may still be accepted. However, providing complete data helps ensure better tracking and treatment.
Although the form is used for reporting, it is best practice to inform patients that their information will be reported, especially for sensitive data.
While healthcare providers typically fill out the form, patients can also inquire about their own health information and reporting if they wish.
The UC 2 form is applicable to all individuals regardless of race, gender, or age. It is designed to collect data from diverse populations.
It is important to note the significant signs and symptoms, but you do not need to list every minor detail. Focus on the most relevant information.
Laboratory results are an essential part of the reporting process. Submitting the form without these results may delay the necessary follow-up actions.
Including treatment information is crucial. It helps healthcare providers understand the patient's history and tailor future care effectively.
By clearing up these misconceptions, individuals and healthcare providers can ensure that they use the Connecticut UC 2 form accurately and effectively.
When filling out and using the Connecticut UC 2 form, it is essential to keep several key points in mind: