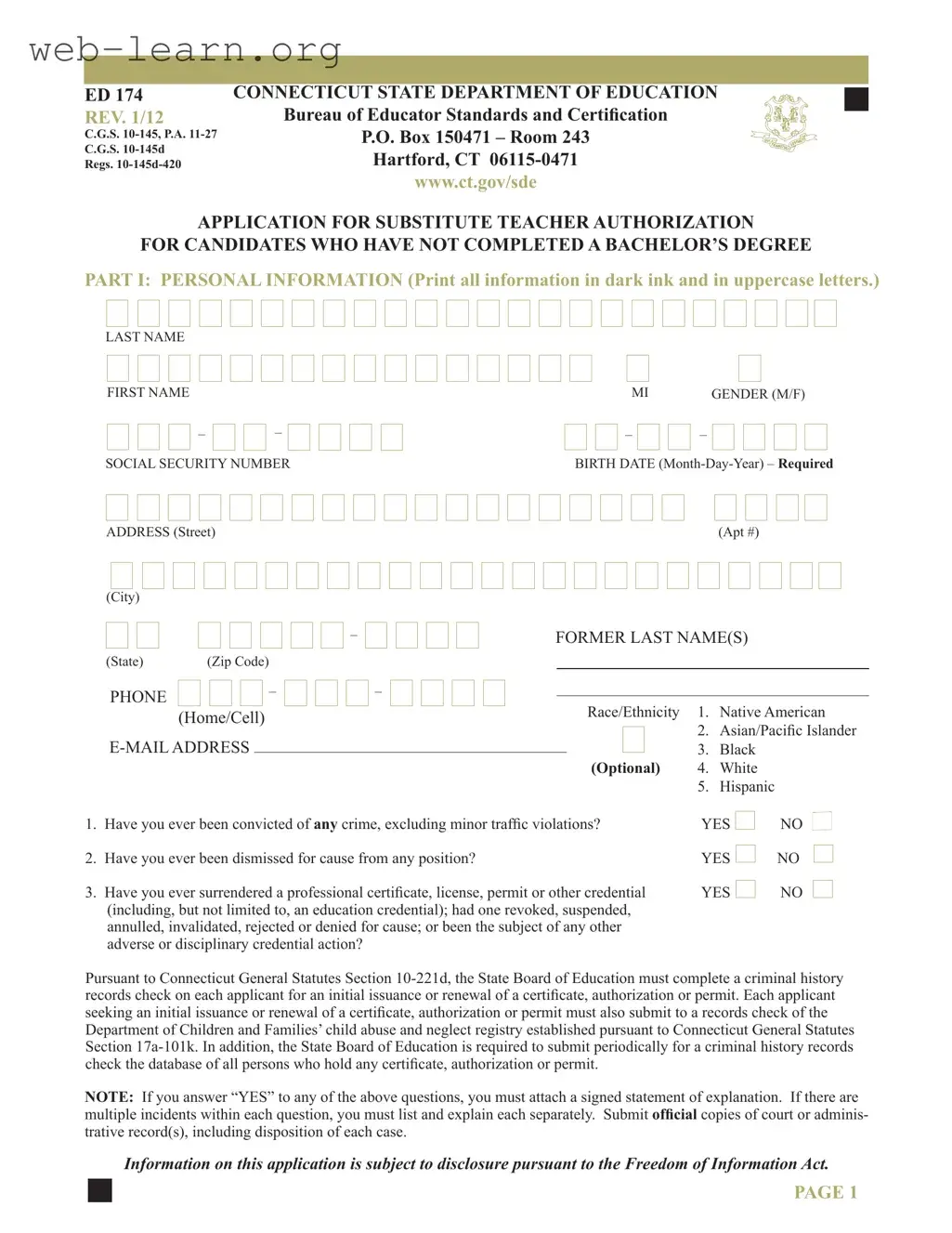
The Connecticut Ed 174 form is a crucial document for individuals seeking to obtain a Substitute Teacher Authorization without having completed a bachelor’s degree. This application encompasses several key components, including personal information, educational background, and attestation of the applicant's qualifications. Applicants must provide details such as their name, contact information, and educational history, along with any relevant experience working with school-age children. Additionally, the form requires candidates to disclose any past criminal convictions or disciplinary actions related to professional credentials, which will be subject to verification through criminal history records checks. The application process also involves an attestation section, where applicants certify the accuracy of their submitted information. Furthermore, the form includes a section for the employing agent, typically a school district official, to verify and endorse the applicant's qualifications. It is essential for applicants to attach a checklist of required documents to ensure their application is complete, as the authorization is valid only until June 30 of the school year in which it is approved. Understanding the intricacies of the Ed 174 form is vital for prospective substitute teachers in Connecticut, as it lays the groundwork for their entry into the educational workforce.
| Fact Name | Details |
|---|---|
| Purpose | The ED 174 form is used to apply for a Substitute Teacher Authorization for candidates who have not completed a bachelor's degree. |
| Governing Laws | This form is governed by Connecticut General Statutes Section 10-145 and Public Act 11-27. |
| Criminal History Check | Applicants must undergo a criminal history records check as required by C.G.S. 10-221d. |
| Expiration | The Substitute Teacher Authorization expires on June 30 of the school year in which it was approved. |
| Application Submission | Completed applications must be returned to the superintendent of schools or their designee for processing. |
Completing the Connecticut Ed 174 form is an essential step for those seeking substitute teacher authorization without a bachelor's degree. The process requires careful attention to detail and the inclusion of various personal and educational information. Following the steps outlined below will ensure that the application is filled out correctly and submitted in a timely manner.
What is the Connecticut Ed 174 form?
The Connecticut Ed 174 form is an application for Substitute Teacher Authorization specifically designed for candidates who have not completed a bachelor’s degree. This form is used to gather personal information, educational background, and relevant experiences of individuals seeking to work as substitute teachers in Connecticut.
Who needs to fill out the Ed 174 form?
Individuals who wish to obtain authorization to work as substitute teachers in Connecticut and have not yet completed a bachelor’s degree must complete the Ed 174 form. This includes those with high school diplomas, GEDs, or other postsecondary education without a degree.
What information is required on the form?
The form requires personal information such as your name, address, date of birth, and social security number. Additionally, you must provide details about your educational background, including schools attended and degrees earned. Any substitute teaching experience or relevant work with school-age children should also be included.
Are there any background checks involved?
Yes, applicants must undergo a criminal history records check as part of the application process. This includes checks against the Department of Children and Families’ child abuse and neglect registry. If you answer "yes" to any questions regarding prior convictions or disciplinary actions, you must provide a signed statement explaining the circumstances.
How long is the Substitute Teacher Authorization valid?
The Substitute Teacher Authorization granted through the Ed 174 form will expire on June 30 of the school year during which it was approved. It is essential to renew the authorization if you wish to continue working as a substitute teacher beyond this date.
What is the process for submitting the Ed 174 form?
First, complete Parts I, II, and III of the form. Afterward, submit the completed application to the superintendent of schools, executive director, or their designee. The employing agent must then complete Part IV and send the application along with any supporting documents to the Bureau of Educator Standards and Certification.
What happens if I provide false information on the form?
Providing false information or failing to disclose relevant details can lead to the denial or revocation of your Substitute Teacher Authorization. It is crucial to ensure that all information provided is accurate and truthful.
Is there a checklist for required documents?
Yes, a checklist must be attached to the completed application packet. This checklist includes all required documents necessary for processing your request for Substitute Teacher Authorization. Make sure to review it thoroughly to ensure all materials are included.
Filling out the Connecticut Ed 174 form can be a straightforward process, but many applicants make mistakes that can delay their application or even lead to denial. One common error is failing to provide complete personal information. Ensure that every section is filled out completely and accurately. For instance, if you leave out your social security number or fail to indicate your gender, it could result in processing delays.
Another frequent mistake is not answering the questions regarding past criminal history and professional conduct accurately. If you answer "YES" to any of these questions, you must attach a signed statement explaining the circumstances. Failing to do so can lead to serious consequences, including the potential denial of your application. It’s crucial to be honest and thorough in this section.
Many applicants also overlook the requirement to list all educational experiences. This includes high school, vocational training, and any postsecondary education. If you skip this section or do not provide complete information about your educational background, your application may be considered incomplete.
Additionally, not providing a resume or separate sheet detailing your substitute teaching experience can be detrimental. This section is essential for showcasing your qualifications and experience working with school-age children. Without this information, decision-makers may not fully understand your suitability for the position.
Lastly, ensure that all signatures are original. The form requires the signature of the superintendent, executive director, or designee. Using a signature stamp is not acceptable. This simple oversight can result in your application being returned for correction, delaying your opportunity to work as a substitute teacher.
When applying for a Substitute Teacher Authorization in Connecticut using the ED 174 form, there are several other documents that may be required to support your application. Each of these documents serves a specific purpose and helps ensure that your application is complete and meets all necessary requirements. Below is a list of commonly used forms and documents that you might need to submit alongside the ED 174 form.
Gathering these documents can seem overwhelming, but each one plays a vital role in your application. Ensuring that you have everything in order will help facilitate a smoother review process and increase your chances of obtaining the necessary authorization to work as a substitute teacher in Connecticut.
When filling out the Connecticut Ed 174 form, it is essential to approach the task with care and attention to detail. Below is a list of things you should and shouldn't do to ensure your application is processed smoothly.
There are several misconceptions surrounding the Connecticut Ed 174 form, which is essential for those seeking authorization to work as substitute teachers without a bachelor's degree. Here are ten common misunderstandings:
Understanding these misconceptions can help applicants navigate the Ed 174 form process more effectively and ensure they meet all necessary requirements for substitute teaching authorization in Connecticut.
Key Takeaways for Filling Out and Using the Connecticut Ed 174 Form