The Concentra Authorization form serves as a critical document for individuals seeking medical examination or treatment, particularly in occupational health settings. This form requires patients to present a photo ID at the time of service, ensuring proper identification. It captures essential personal information, including the patient’s name, social security number, employer, and date of birth, which helps in maintaining accurate medical records. The form outlines various examination types, such as work-related physical examinations, DOT physicals, and substance abuse testing, allowing patients to specify the nature of their visit. Additionally, patients can indicate whether the examination is for preplacement, annual, or exit purposes, among others. The form also addresses billing considerations, including options for employee payment and post-accident assessments. Special instructions and comments sections provide space for any additional notes that may be relevant to the patient's situation. Notably, Concentra emphasizes that only the patient and medical staff are permitted in the testing area, underscoring the importance of privacy and focus during the examination process. Furthermore, the form reflects Concentra's commitment to providing urgent care services for non-work-related illnesses and injuries, and it highlights the acceptance of various insurance plans, making healthcare more accessible. Copies of this form can be conveniently accessed online, ensuring that patients can prepare for their appointments effectively.

| Fact Name | Description |
|---|---|
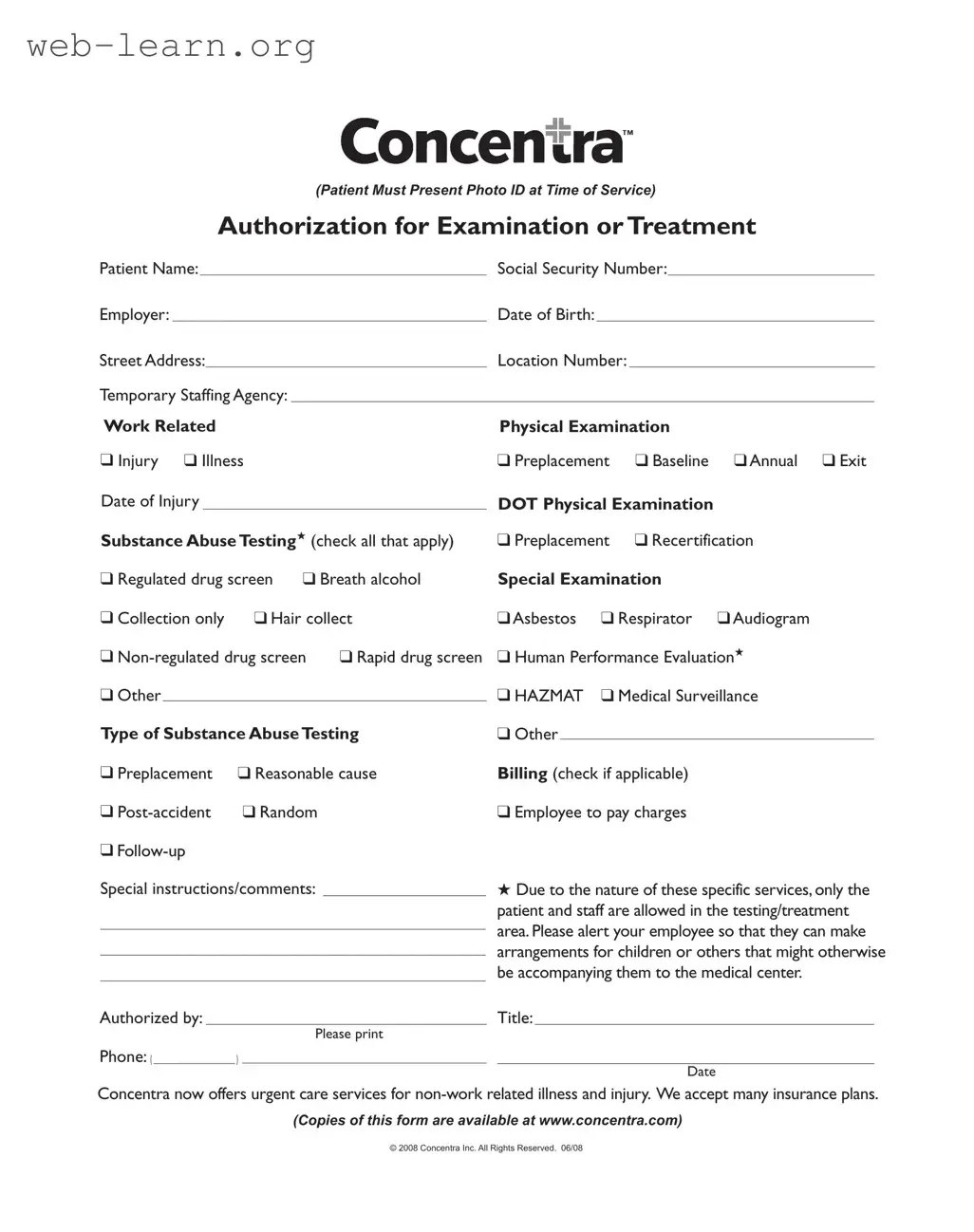
| Patient ID Requirement | Patients must present a photo ID at the time of service to be eligible for examination or treatment. |
| Authorization Scope | The form authorizes various types of examinations, including work-related physicals, DOT physicals, and substance abuse testing. |
| Billing Responsibility | Patients can indicate if they will pay charges, especially for post-accident or random testing. |
| Special Instructions | Patients can provide comments or special instructions, which may be crucial for their treatment. |
| Privacy in Testing Area | Only the patient and staff are allowed in the testing area to ensure privacy and focus during examinations. |
Completing the Concentra Authorization form is an important step in the process of receiving medical examination or treatment. This form gathers essential information that will facilitate your visit. It is important to ensure that all sections are filled out accurately to avoid any delays in service.
Once you have completed the form, ensure that you bring a photo ID with you at the time of service. This will help verify your identity and facilitate a smooth process during your visit.
What is the purpose of the Concentra Authorization form?
The Concentra Authorization form is designed to grant permission for medical examinations or treatments related to work-related injuries, illnesses, or other specified services. It ensures that the medical staff can proceed with the necessary evaluations and tests after obtaining the patient's consent. The form includes sections for identifying the patient, the nature of the examination, and any specific instructions or comments from the employer or the patient.
What information do I need to provide on the form?
When filling out the Concentra Authorization form, you will need to provide several key pieces of information, including:
Additionally, you must present a photo ID at the time of service to verify your identity.
What types of examinations and tests are covered by this form?
The Concentra Authorization form covers a variety of examinations and tests. These may include:
Patients can select the specific tests they require by checking the appropriate boxes on the form.
What should I do if I have questions or need assistance with the form?
If you have any questions or need help while completing the Concentra Authorization form, it is advisable to reach out to the medical center staff. They are trained to assist you with the form and can provide guidance on any specific requirements. Additionally, you can visit the Concentra website for further information and access to copies of the form.
Filling out the Concentra Authorization form can seem straightforward, but many individuals make common mistakes that can lead to delays or complications in receiving care. Here are nine frequent errors to avoid when completing this important document.
First, one of the most critical mistakes is failing to present a photo ID at the time of service. This requirement is not optional; without proper identification, the process can be halted. Ensure that you have your ID ready before arriving at the medical center.
Another common error is neglecting to provide accurate personal information. The form requires your full name, Social Security number, and date of birth. Missing or incorrect details can lead to confusion and delays in processing your authorization.
People often overlook the employer's name section. It is essential to include the correct employer information to ensure that the services are billed appropriately. Double-check the spelling and accuracy of the employer's name to avoid any issues.
Additionally, many individuals fail to specify the type of examination or treatment they are seeking. The form includes various options, such as work-related physical examinations and substance abuse testing. Marking the correct boxes is vital to ensure that the appropriate services are rendered.
Another frequent mistake involves the billing section. Some people forget to check applicable billing options, such as whether the employee will pay charges. This oversight can lead to unexpected costs and confusion regarding payment responsibilities.
Additionally, leaving the special instructions or comments section blank can be a missed opportunity to communicate important information. If there are specific needs or circumstances that the medical staff should know, be sure to include them in this section.
People sometimes forget to sign the form or provide their printed name. An unsigned form is not valid, and without a printed name, it can be challenging for staff to identify who authorized the treatment. Always ensure that both your signature and printed name are included.
It is also common for individuals to neglect to provide a contact phone number. This information is crucial for follow-up communications or if any issues arise during the treatment process. Make sure to include a reliable phone number where you can be reached.
Lastly, some individuals may not be aware of the specific services offered by Concentra. Familiarizing yourself with the range of services available can help you select the right options on the form, ensuring that you receive the care you need without unnecessary delays.
By avoiding these common mistakes, you can streamline the process of filling out the Concentra Authorization form and ensure that your medical needs are met efficiently.
When utilizing the Concentra Authorization form, several other documents may be required to ensure comprehensive care and compliance with regulations. Each of these documents serves a specific purpose in the healthcare and employment process. Below is a list of commonly associated forms and documents.
These documents work together to create a thorough and efficient process for patient care and administrative compliance. Ensuring that all necessary forms are completed accurately helps facilitate a smoother experience for both patients and healthcare providers.
The Concentra Authorization form is an important document that grants permission for medical examination or treatment. Several other documents share similar purposes and structures. Here are five such documents:
Filling out the Concentra Authorization form accurately is crucial for ensuring a smooth experience during your medical examination or treatment. Here are five essential dos and don'ts to keep in mind:
Misconceptions about the Concentra Authorization form can lead to confusion and complications for patients. Here are six common misunderstandings:
When filling out the Concentra Authorization form, there are several important points to keep in mind. Here are key takeaways to ensure a smooth process:
Following these guidelines will help facilitate your experience at Concentra and ensure that all necessary information is provided for your care.