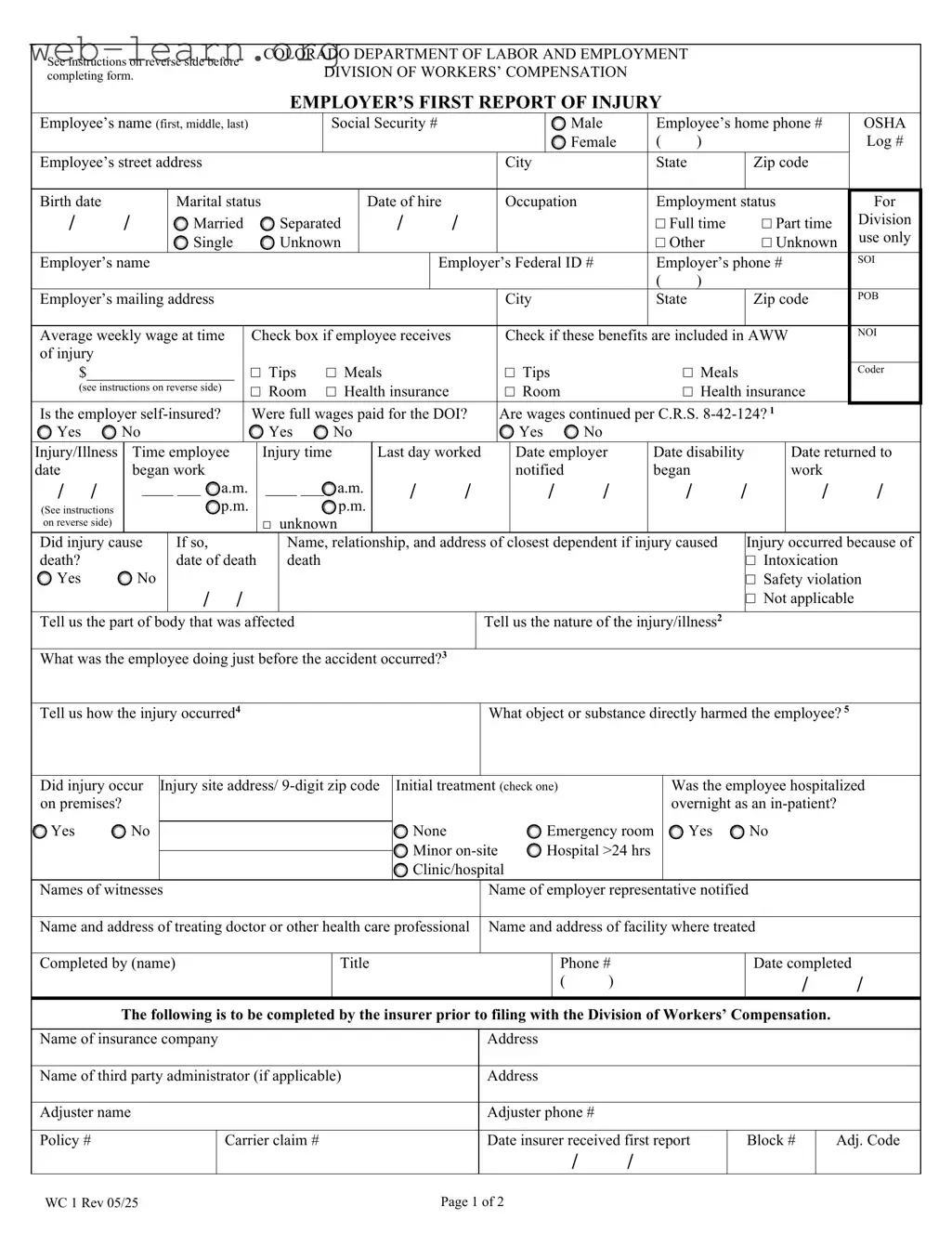
The Colorado WC 1 form, known as the Employer’s First Report of Injury, is a crucial document in the workers' compensation process. This form serves as the initial report that employers must submit to their insurance carriers following an employee's work-related injury or illness. It captures essential information about the injured employee, including their name, address, and social security number, as well as details about the employer and the nature of the injury. The form requires specifics such as the date of the injury, the last day worked, and whether the injury resulted in death. Additionally, it gathers information about the circumstances surrounding the injury, including what the employee was doing at the time and how the injury occurred. Employers must also disclose the average weekly wage of the employee, which can influence compensation calculations. It is important to note that all injuries, regardless of severity, must be reported, particularly those leading to lost time from work. Failure to comply with these reporting requirements can have significant implications for both the employer and the injured employee. By understanding the components and requirements of the WC 1 form, employers can ensure they fulfill their obligations under Colorado's workers' compensation laws, ultimately supporting their employees during a challenging time.
| Fact Name | Description |
|---|---|
| Form Purpose | The Colorado WC 1 form is used to report work-related injuries or illnesses to the employer's insurance carrier. |
| Governing Law | The form is governed by the Colorado Workers' Compensation Act, specifically C.R.S. 8-42-124. |
| Reporting Timeframe | Injuries that result in lost time must be reported within ten days of notice or knowledge of the injury. |
| Injury Types | All injuries, regardless of severity, must be reported, including occupational diseases and fatalities. |
| Employee Information | The form requires detailed employee information, including name, address, Social Security number, and employment status. |
| Employer Responsibilities | Employers must select the physician for the injured employee's treatment and report injuries promptly. |
| Average Weekly Wage Calculation | The average weekly wage is calculated by considering overtime, tips, and other benefits provided by the employer. |
| Witness Information | The form allows for the inclusion of witnesses to the injury, which can be crucial for claims processing. |
| Penalties for Misrepresentation | Providing false information on the form can lead to penalties, including fines and imprisonment, as stated in C.R.S. 10-1-128(6)(a). |
Filling out the Colorado WC 1 form is an essential step in reporting a workplace injury. Accurate completion of this form ensures that all necessary information is provided for the employer's insurance carrier. Follow these steps carefully to ensure the form is filled out correctly.
What is the Colorado WC 1 form?
The Colorado WC 1 form, also known as the Employer’s First Report of Injury, is a document that employers must complete to report workplace injuries or illnesses. This form is essential for initiating a claim for workers' compensation benefits and must be submitted to the insurance carrier within a specific timeframe after an injury occurs.
When should the WC 1 form be filed?
Employers must file the WC 1 form within ten days after they are notified of an injury or illness that results in lost time from work exceeding three shifts or calendar days. If the injury results in death, the form must be submitted immediately.
What information is required on the WC 1 form?
The form requires detailed information about the employee, including their name, address, Social Security number, date of hire, and employment status. Additionally, it asks for specifics about the injury, such as the date it occurred, the nature of the injury, and the circumstances surrounding the accident.
How do I calculate the Average Weekly Wage (AWW)?
To calculate the AWW, add the employee's regular weekly wage to any average weekly overtime, tips, or commissions. If the employer provides benefits like housing or health insurance that will not continue during the disability period, include their average weekly value in the calculation. The total should be recorded in the designated field on the form.
What happens if the injury leads to death?
If the injury causes death, the form must indicate this, and the employer should provide the name, relationship, and address of the closest dependent. This information is crucial for the processing of any death benefits that may be applicable.
Can employers choose the treating physician?
Yes, under Colorado law, employers have the right to select the physician who will treat the injured employee. This is an important aspect of managing workers' compensation claims effectively.
What if the employee was intoxicated at the time of the injury?
If the injury occurred due to intoxication, this should be noted on the form. Intoxication can affect the eligibility for benefits, so it’s essential to provide accurate information regarding the circumstances of the injury.
What are the consequences of providing false information?
Providing false, incomplete, or misleading information on the WC 1 form is unlawful and can result in severe penalties. This includes potential imprisonment, fines, or denial of insurance claims. It’s crucial to ensure that all information is accurate and truthful.
How should the WC 1 form be submitted?
The completed form should be submitted to the employee’s insurance carrier. It is recommended to keep a copy for your records. Ensure that the form is filled out legibly and completely to avoid delays in processing the claim.
Completing the Colorado WC 1 form accurately is crucial for ensuring that workers' compensation claims are processed smoothly. One common mistake is failing to provide complete and accurate personal information. For instance, if the employee’s name or Social Security number is incorrect, it can lead to delays or even denial of benefits. Always double-check that all names are spelled correctly and that all identification numbers are accurate.
Another frequent error occurs in the section regarding the average weekly wage. Many individuals miscalculate this figure, which can have significant implications for the benefits the employee may receive. It is essential to include not only the base salary but also any overtime, tips, or other compensation that may apply. Neglecting to factor in these additional earnings can result in an inadequate compensation amount, impacting the employee’s financial stability during recovery.
People often overlook the importance of providing detailed information about the injury itself. Vague descriptions can lead to misunderstandings and complications in the claims process. For example, instead of simply stating “hurt back,” it is better to specify the nature of the injury, such as “strained lower back while lifting a heavy box.” Clear and specific descriptions help in accurately assessing the situation and determining the appropriate benefits.
Additionally, some individuals fail to check all relevant boxes in the form. Each checkbox serves a purpose and provides necessary information for the claim. Skipping these can create gaps in the report, leading to further inquiries and delays. It is advisable to carefully review each section and ensure that all applicable boxes are checked before submission.
Lastly, many people neglect to keep a copy of the completed form for their records. This oversight can create difficulties if there are questions or disputes later on. Retaining a copy ensures that both the employee and the employer have access to the information submitted, which can be invaluable for follow-up communications. Keeping thorough records is always a best practice in any legal or administrative process.
When dealing with workplace injuries in Colorado, the WC 1 form, or the Employer's First Report of Injury, is just one piece of the puzzle. Several other forms and documents are often required to ensure that all aspects of the workers' compensation process are properly addressed. Here’s a brief overview of five commonly used documents that accompany the WC 1 form.
Understanding these documents can significantly streamline the workers' compensation process. Each form serves a specific purpose, ensuring that both the employer and employee have a clear understanding of the situation and the steps that need to be taken. Properly managing these forms can help facilitate timely compensation and support for injured workers.
The Colorado WC 1 form is a crucial document for reporting workplace injuries. Several other forms serve similar purposes in different contexts. Here’s a list of ten documents that share similarities with the Colorado WC 1 form:
When completing the Colorado WC 1 form, attention to detail is crucial. Here are some key dos and don'ts to ensure the process goes smoothly.
By following these guidelines, you can help facilitate a smoother reporting process and ensure compliance with state regulations.
Here are five misconceptions about the Colorado WC 1 form that need clarification:
When filling out the Colorado WC 1 form, it’s important to keep several key points in mind:
By following these guidelines, you can help ensure that the process runs smoothly and that all necessary information is provided for a timely response from your insurance carrier.