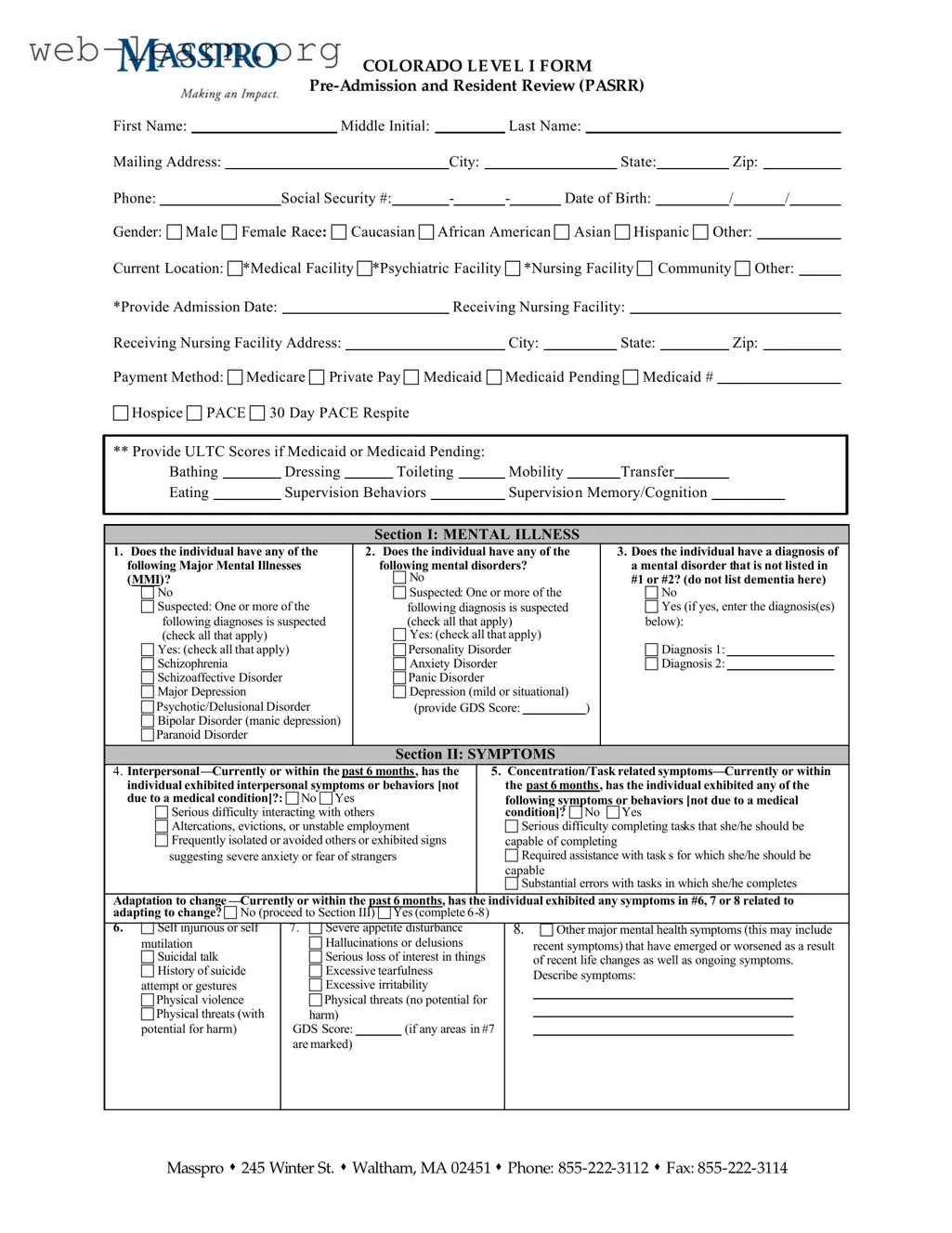
The Colorado Post Admission Level 1 PASRR form serves as a critical tool for assessing individuals who may require specialized care in nursing facilities. This form collects essential personal information, including the individual's name, date of birth, and social security number, alongside their current location and payment method. It also addresses various mental health conditions and symptoms, allowing for a comprehensive evaluation of the individual's mental health history. Sections of the form specifically inquire about diagnoses related to mental illnesses, symptoms exhibited in the past six months, and any history of psychiatric treatment. Additionally, the form assesses cognitive impairments and the presence of developmental disabilities. It includes important questions regarding exemptions and categorical decisions, which must be approved prior to admission. The outcome section of the form determines whether further screening is necessary based on the responses provided. Overall, the Colorado Post Admission Level 1 PASRR form is a vital component in ensuring that individuals receive the appropriate level of care tailored to their specific needs.

| Fact Name | Description |
|---|---|
| Form Purpose | The Colorado Post Admission Level 1 PASRR form is designed to assess individuals for mental illness or developmental disabilities prior to admission to a nursing facility. |
| Governing Law | This form is governed by the federal PASRR regulations under the Omnibus Budget Reconciliation Act (OBRA) of 1987 and Colorado state law. |
| Submission Requirements | Completed forms must be submitted to Masspro within specified time frames to ensure timely review and approval for nursing facility admissions. |
| Key Sections | The form includes critical sections such as mental illness assessment, history of psychiatric treatment, and exemptions for specific conditions. |
| Importance of Accuracy | Accurate completion of the form is essential, as it directly impacts eligibility for services and the level of care required by the individual. |
Completing the Colorado Post Admission Level 1 Passr form is a crucial step in the admission process for individuals requiring specific care. This form gathers essential information about the individual’s mental health status, treatment history, and current living situation. Once filled out, the form will be submitted to the appropriate authorities for review and processing.
What is the Colorado Post Admission Level 1 PASRR form?
The Colorado Post Admission Level 1 PASRR form is a standardized document used to assess individuals with mental illness or developmental disabilities who are being admitted to nursing facilities. The form collects essential information about the individual's medical history, current condition, and any prior psychiatric treatments to determine their eligibility for services and support.
Who needs to complete the PASRR form?
The PASRR form must be completed for individuals who are being admitted to a nursing facility and are suspected of having a mental illness or developmental disability. This requirement applies to all potential residents to ensure they receive appropriate care and services tailored to their needs.
What information is required on the PASRR form?
The form requires various details, including:
How does the PASRR process work?
Once the PASRR form is completed, it is submitted to Masspro, the organization responsible for reviewing the information. They assess whether the individual meets the criteria for further evaluation or services. If further screening is necessary, additional information may be requested.
What happens if an individual does not meet the criteria for further screening?
If the individual does not meet the criteria for further screening, the PASRR process concludes. The facility can proceed with the admission, and no additional assessments are required.
What are the potential outcomes of the PASRR assessment?
The outcomes can include:
How is confidentiality maintained during the PASRR process?
Confidentiality is a critical component of the PASRR process. The information collected is protected under HIPAA regulations, ensuring that personal health information is only shared with authorized individuals involved in the assessment and care of the individual.
What should be done if there are changes in the individual's condition after submission?
If there are significant changes in the individual's mental or physical condition after the PASRR form has been submitted, it is essential to notify the nursing facility and Masspro. This information may impact the individual's care plan and eligibility for services.
Where can I get assistance with completing the PASRR form?
Assistance with completing the PASRR form can be obtained from healthcare professionals, social workers, or the admissions office of the nursing facility. Additionally, Masspro provides resources and support for individuals and families navigating the PASRR process.
Filling out the Colorado Post Admission Level 1 PASRR form requires careful attention to detail. One common mistake is failing to provide complete personal information. Individuals often leave out essential details such as the middle initial or the full mailing address. This omission can delay the processing of the application and may lead to complications in the admission process.
Another frequent error is the incomplete selection of payment methods. Applicants may forget to check the appropriate box for their payment source, whether it be Medicare, Medicaid, or private pay. This oversight can create confusion regarding financial responsibilities and eligibility for services.
In Section I, individuals sometimes do not clearly indicate the presence of mental illnesses or disorders. Failing to check the appropriate boxes or providing vague responses can result in an inaccurate assessment of the individual's mental health status. It is crucial to be as specific as possible when noting diagnoses and symptoms.
Additionally, applicants often overlook the need to provide supporting documentation for diagnoses listed in the form. For instance, if a diagnosis of dementia is indicated, corroborative testing information should be included. Without this information, the review process may be stalled.
Another mistake involves the failure to list all prescribed medications accurately. In Section V, individuals may neglect to mention psychoactive medications that were taken within the past six months. This could lead to an incomplete understanding of the individual's treatment history and current needs.
Many applicants also misinterpret the questions regarding psychiatric treatment history. Some may fail to disclose significant life disruptions or previous mental health services, which could influence the evaluation of the individual’s current mental health status. Transparency in this section is vital for appropriate care.
Moreover, individuals sometimes do not check for exemptions or categorical decisions accurately. Misunderstanding the criteria for hospital exemption or terminal illness can lead to incorrect submissions. It is essential to review the requirements thoroughly before marking these sections.
Lastly, applicants may neglect to sign and date the form. This final step is crucial, as an unsigned form may be considered invalid, causing delays in processing. Ensuring all sections are completed, reviewed, and signed is necessary for a smooth admission process.
The Colorado Post Admission Level 1 PASRR form is a critical document used to assess individuals before their admission to certain healthcare facilities. It gathers essential information about the individual's mental health status, history, and current needs. Several other forms and documents complement this process to ensure a comprehensive evaluation and appropriate care. Below is a list of these documents, each serving a specific purpose in the admission process.
These documents collectively contribute to a thorough understanding of the individual's needs and ensure that appropriate care is provided from the moment of admission. Timely completion and submission of these forms can significantly impact the quality of care and support the individual receives.
The Colorado Post Admission Level 1 PASRR form is a critical document used in assessing individuals for mental health and developmental disabilities prior to admission to certain facilities. There are several other documents that share similarities with this form in terms of purpose and structure. Here are five comparable documents:
When filling out the Colorado Post Admission Level 1 PASRR form, it’s essential to approach the task with care and attention. Here’s a list of ten things to keep in mind:
Following these guidelines can help ensure that the form is filled out correctly and efficiently, facilitating a smoother admission process.
Understanding the Colorado Post Admission Level 1 PASRR form is crucial for ensuring proper care and compliance. However, several misconceptions exist regarding its purpose and use. Here are six common misconceptions:
Being aware of these misconceptions can help ensure that the PASRR process is navigated correctly, leading to appropriate care and support for individuals in need.
Filling out the Colorado Post Admission Level 1 PASRR form is a crucial step in ensuring appropriate care for individuals with mental health needs. Here are some key takeaways to keep in mind:
By paying attention to these details, you can help ensure that the individual receives the necessary evaluations and services they require.