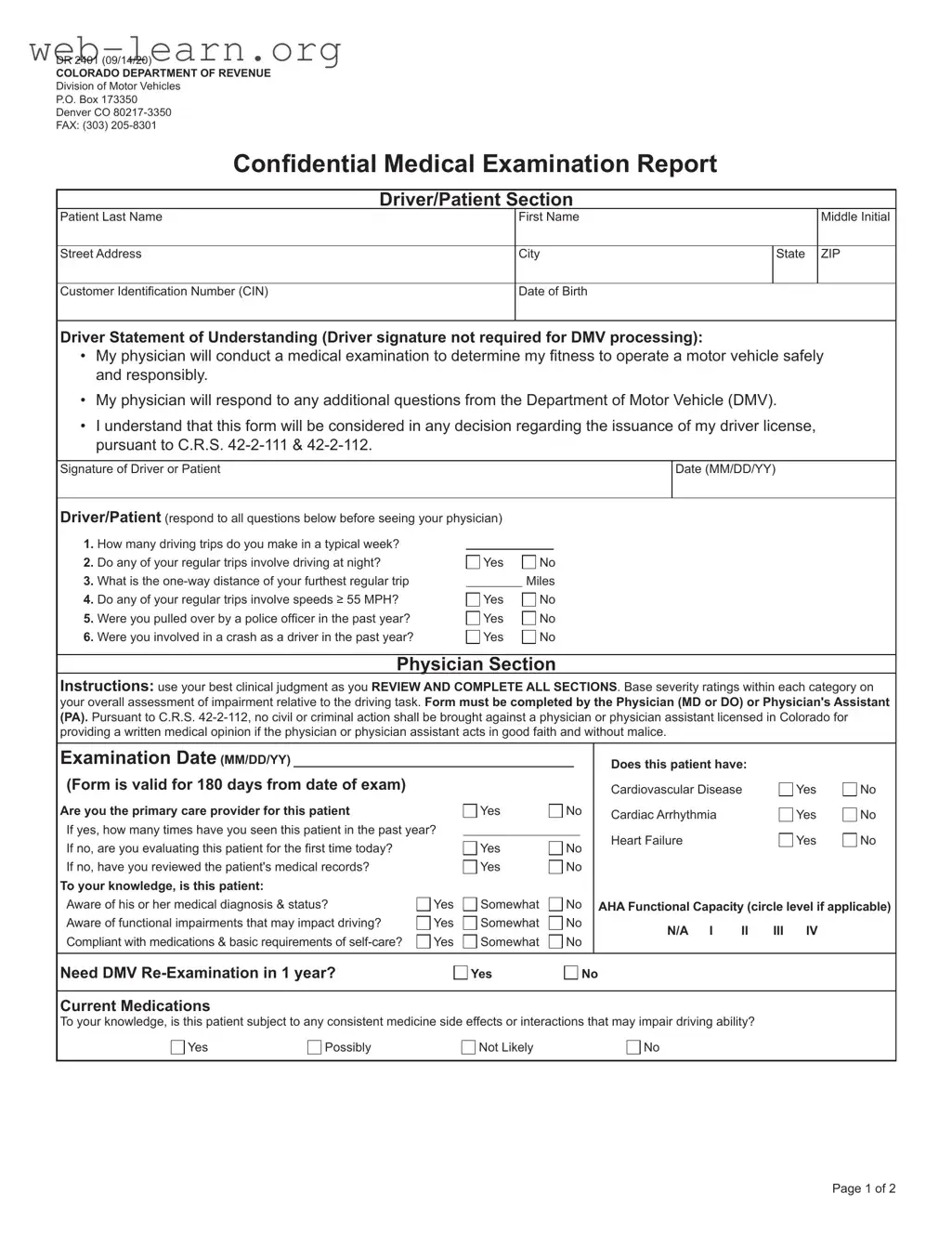
The Colorado DR 2401 form serves a crucial role in ensuring that individuals who wish to operate a motor vehicle are medically fit to do so. This form is designed for use by both drivers and their physicians, facilitating a comprehensive medical examination that assesses various health factors impacting driving ability. The form includes sections for the driver to provide personal information, such as their name, address, and date of birth, along with a statement of understanding regarding the medical evaluation. In this statement, the driver acknowledges that their physician will assess their fitness to drive and that the findings will be considered by the Department of Motor Vehicles (DMV) in any licensing decisions. The physician's section of the form requires a thorough evaluation of the patient's medical history, including conditions related to cardiovascular health, cognitive function, and any psychiatric issues that may affect driving. Physicians are guided to use their clinical judgment to determine the patient's fitness level and recommend any necessary restrictions, such as daylight driving only or the need for further testing. The form is valid for 180 days from the examination date, emphasizing the importance of up-to-date medical assessments in safeguarding public safety on the roads.
| Fact Name | Description |
|---|---|
| Form Purpose | The DR 2401 form is a Confidential Medical Examination Report used to assess a driver's fitness to operate a motor vehicle safely. |
| Governing Laws | This form is governed by Colorado Revised Statutes (C.R.S.) 42-2-111 and 42-2-112, which outline the requirements for medical evaluations related to driving. |
| Validity Period | The medical examination results are valid for 180 days from the date of the exam, ensuring timely assessments of a driver's capabilities. |
| Completion Requirement | The form must be completed by a licensed physician (MD or DO) or a physician's assistant (PA) to ensure professional evaluation. |
| Driver Statement | Drivers must acknowledge their understanding of the medical examination process, indicating their awareness of its implications for their driving privileges. |
| Confidentiality Clause | The form includes a confidentiality provision, protecting physicians from civil or criminal liability when providing medical opinions in good faith. |
| Patient Information | Patients must provide personal details, including their last name, first name, middle initial, address, and date of birth, ensuring accurate identification. |
| Assessment Areas | The form assesses various health conditions, including cardiovascular, neurological, and psychiatric issues, which may impact driving ability. |
Completing the Colorado DR 2401 form is a critical step in ensuring a thorough medical evaluation for driving fitness. This form requires information from both the driver and the physician. Following the steps below will help ensure that all necessary information is accurately provided.
After completing the form, it should be submitted to the appropriate DMV office for processing. Ensure that both sections are filled out completely to avoid delays in the review process.
The Colorado DR 2401 form is a Confidential Medical Examination Report that assesses a driver's fitness to operate a motor vehicle safely. It is primarily used by the Department of Motor Vehicles (DMV) to evaluate whether an individual meets the necessary medical standards for holding a driver’s license. The form collects information from both the driver and their physician, ensuring that all relevant health factors are considered in the licensing process.
The form must be completed by a licensed physician (MD or DO) or a physician's assistant (PA). The medical professional must conduct a thorough examination and provide their assessment based on the driver's medical history and current health status. It is essential that the physician uses their best clinical judgment when filling out the form.
Before seeing their physician, the driver must answer several questions on the form. These include:
These questions help the physician assess the driver’s overall driving habits and potential risks.
The form is valid for 180 days from the date of the medical examination. After this period, a new examination and form submission will be necessary for the DMV to consider the driver’s medical fitness for operating a vehicle.
Filling out the Colorado DR 2401 form can be a straightforward process, but there are common mistakes that can lead to delays or complications. One frequent error is failing to answer all the questions in the Driver/Patient section. This section is crucial as it provides the physician with necessary information about your driving habits and health status. Omitting answers can result in an incomplete assessment, which may hinder your ability to obtain or maintain your driver’s license.
Another common mistake is neglecting to provide accurate personal information. This includes your full name, address, and date of birth. Inaccurate details can create confusion and may even lead to processing delays. Always double-check that all personal information matches your identification documents to avoid any issues.
People often overlook the importance of the physician's section. It must be completed thoroughly by a licensed physician or physician's assistant. If the physician fails to review the patient’s medical records or does not provide a detailed assessment, it could compromise the validity of the form. This oversight can result in the need for additional evaluations or even denial of your application.
Lastly, many individuals do not pay attention to the expiration of the form. The DR 2401 is only valid for 180 days from the examination date. If you submit the form after this period, it will not be accepted. Make sure to keep track of the examination date and submit your form promptly to ensure it is processed without delays.
The Colorado DR 2401 form is a critical document used for assessing a driver's medical fitness to operate a motor vehicle. Along with this form, several other documents and forms are commonly utilized in the process of medical evaluations and licensing. Each of these plays a unique role in ensuring that drivers meet safety standards. Below is a list of forms that are often associated with the DR 2401, providing a brief description of each.
In conclusion, these forms collectively support the goal of maintaining safe driving standards across Colorado. Each document serves a specific purpose, contributing to a comprehensive evaluation of a driver's fitness to operate a vehicle. Understanding these forms can help individuals navigate the process more effectively and ensure compliance with state regulations.
The Colorado DR 2401 form serves a specific purpose in assessing a driver's medical fitness to operate a vehicle. Several other documents share similarities with this form, each catering to different contexts but fundamentally aiming to evaluate an individual's health status in relation to driving. Below is a list of nine documents that are comparable to the Colorado DR 2401 form:
These documents, while varying in specific focus and detail, all share the common goal of ensuring that individuals are medically fit to drive, thereby promoting road safety for everyone.
When filling out the Colorado DR 2401 form, it is crucial to follow specific guidelines to ensure accuracy and compliance. Here are six essential do's and don'ts to consider:
Misconceptions about the Colorado DR 2401 form can lead to confusion regarding its purpose and requirements. Here are ten common misunderstandings:
Here are key takeaways regarding the Colorado DR 2401 form: