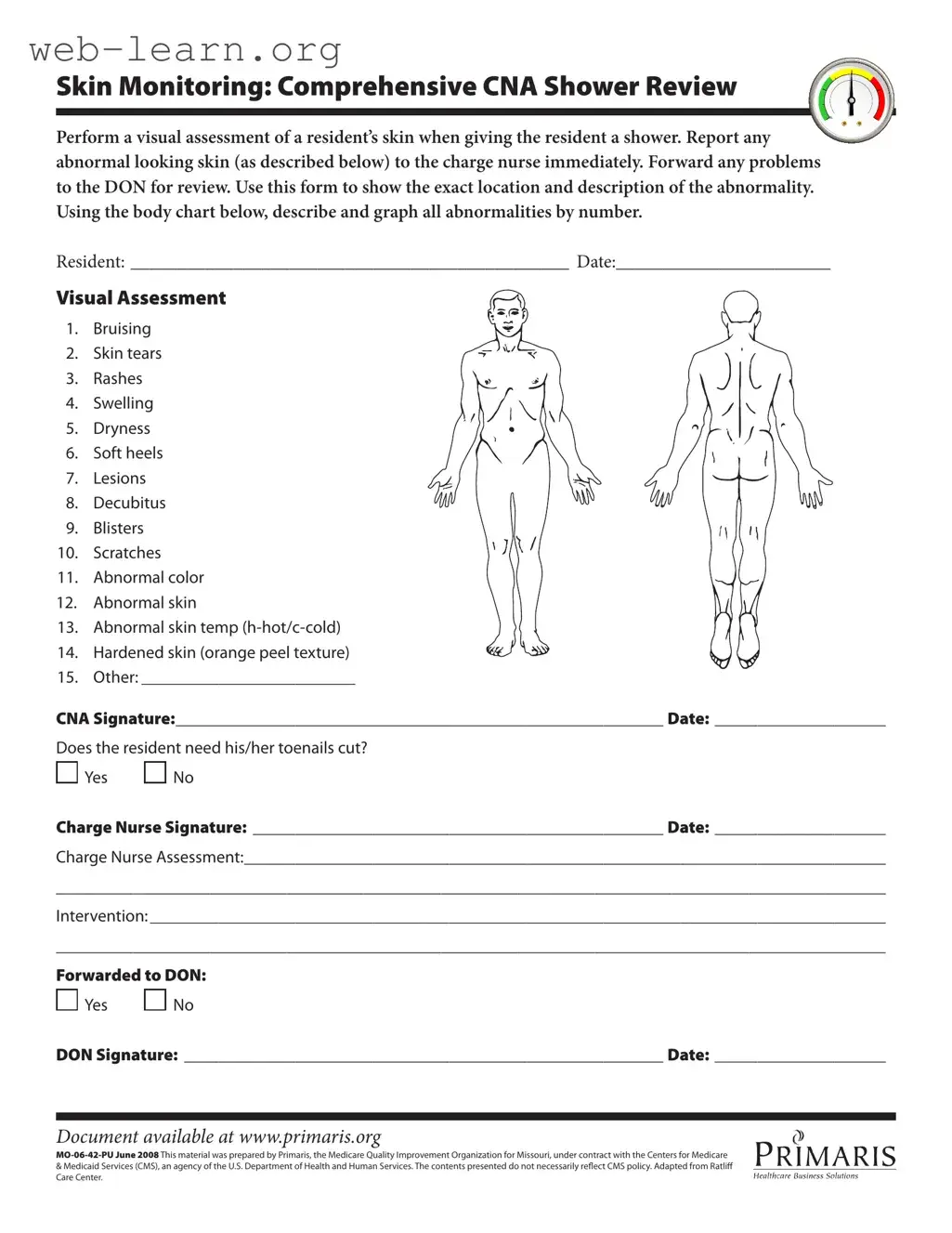
The CNA Shower Sheets form is an essential tool for ensuring the health and safety of residents during their showering experience. This form guides Certified Nursing Assistants (CNAs) in conducting a thorough visual assessment of a resident's skin while providing care. It covers various aspects of skin monitoring, including identifying and documenting any abnormalities such as bruising, skin tears, rashes, and lesions. CNAs are instructed to report any concerning findings to the charge nurse immediately, facilitating prompt intervention. The form also includes a body chart for CNAs to accurately mark the location of any abnormalities, ensuring clear communication among the care team. Additionally, it prompts the CNA to assess whether the resident needs toenail care, further enhancing their overall well-being. After the initial assessment, the charge nurse reviews the findings, adds their signature, and may forward any concerns to the Director of Nursing (DON) for further evaluation. This structured approach not only promotes accountability but also supports the ongoing health monitoring of residents, making it a vital component of quality care.
| Fact Name | Description |
|---|---|
| Purpose | The CNA Shower Sheets form is designed for documenting skin assessments during resident showers. |
| Assessment Areas | It includes a visual assessment of various skin conditions such as bruising, rashes, and lesions. |
| Reporting Protocol | Any abnormalities must be reported to the charge nurse immediately and forwarded to the Director of Nursing (DON) for review. |
| Signature Requirement | The form requires signatures from both the CNA and the charge nurse to validate the assessment. |
| State-Specific Law | In Missouri, this form is governed by state regulations regarding resident care and documentation standards. |
Completing the CNA Shower Sheets form requires careful attention to detail. This form is essential for documenting the skin condition of residents during showers. Follow the steps below to ensure accurate and thorough completion of the form.
The CNA Shower Sheets form is designed to assist Certified Nursing Assistants (CNAs) in conducting thorough skin assessments during resident showers. It serves as a tool for documenting any abnormalities observed on a resident’s skin, such as bruising, rashes, or lesions. This documentation is essential for ensuring that any issues are promptly reported to the charge nurse and subsequently reviewed by the Director of Nursing (DON).
If a CNA identifies any abnormal skin conditions while giving a shower, they must report these findings to the charge nurse immediately. The form allows for the precise location and description of the abnormality to be recorded. This information is crucial for the charge nurse to evaluate the situation and determine any necessary interventions.
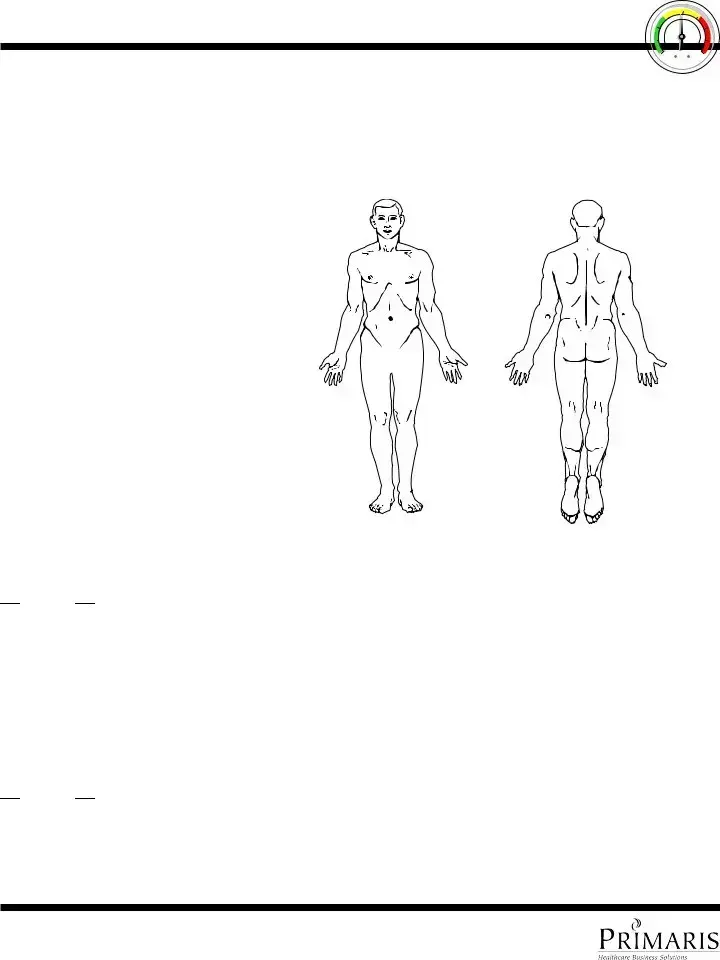
The form includes a visual assessment section where CNAs can check off various skin conditions observed during the shower. Each abnormality is numbered, and CNAs are required to describe and graph these findings on a body chart provided within the form. This structured documentation helps maintain a clear record of the resident's skin condition over time.
Once the charge nurse completes their assessment, they will document their findings and any recommended interventions on the form. If necessary, the charge nurse may forward the information to the DON for further review. The form also includes a section to indicate whether the resident requires toenail care, ensuring that all aspects of the resident's well-being are addressed.
Filling out the CNA Shower Sheets form is an essential task that helps ensure residents receive the proper care they need. However, many individuals make mistakes that can lead to serious consequences. One common error is failing to provide complete information about the resident. It's crucial to fill in all sections, including the resident's name and the date. Omitting this basic information can cause confusion and delay in addressing any issues that may arise.
Another mistake is not accurately documenting the findings during the visual assessment. The form includes specific categories for skin conditions, such as bruising, rashes, and swelling. Skipping these details or providing vague descriptions can hinder the charge nurse's ability to make informed decisions about the resident's care. Always take the time to thoroughly assess the skin and record what you observe.
Additionally, many people forget to sign and date the form. This step is not just a formality; it serves as a record of accountability. Without a signature, it can be challenging to trace back who conducted the assessment or when it was completed. This lack of documentation can lead to misunderstandings or disputes regarding the care provided.
Lastly, neglecting to communicate any abnormalities to the charge nurse promptly is a significant oversight. If you notice something unusual during the shower, such as a skin tear or lesion, it's essential to report it immediately. Delaying this communication can result in further complications for the resident. Always remember that timely reporting can make a difference in the quality of care provided.
The CNA Shower Sheets form is an essential document for monitoring residents' skin health during showers. However, several other forms and documents complement this process, ensuring comprehensive care and documentation. Below is a list of these related documents, each serving a specific purpose in the care continuum.
These forms and documents work together to create a holistic approach to resident care. By maintaining thorough and accurate records, healthcare providers can ensure that each resident receives the attention and support they need for optimal health and well-being.
The CNA Shower Sheets form is essential for documenting skin assessments during resident showers. Several other documents serve similar purposes in healthcare settings, focusing on patient monitoring and care. Here’s a list of eight documents that share similarities with the CNA Shower Sheets:
Each of these documents plays a vital role in ensuring comprehensive care and monitoring of residents, emphasizing the importance of thorough documentation in healthcare settings.
When filling out the CNA Shower Sheets form, it is important to follow certain guidelines to ensure accuracy and clarity. Below is a list of things you should and shouldn't do while completing this form.
By adhering to these guidelines, you can help ensure that the resident's skin health is accurately monitored and reported. This attention to detail is crucial for providing the best care possible.
Misconceptions about the CNA Shower Sheets form can lead to misunderstandings regarding its purpose and use. Below are five common misconceptions along with clarifications.
Filling out and using the CNA Shower Sheets form is an important task for ensuring resident care. Here are some key takeaways to keep in mind:
By following these guidelines, you can help maintain the health and safety of residents, ensuring they receive the best possible care.