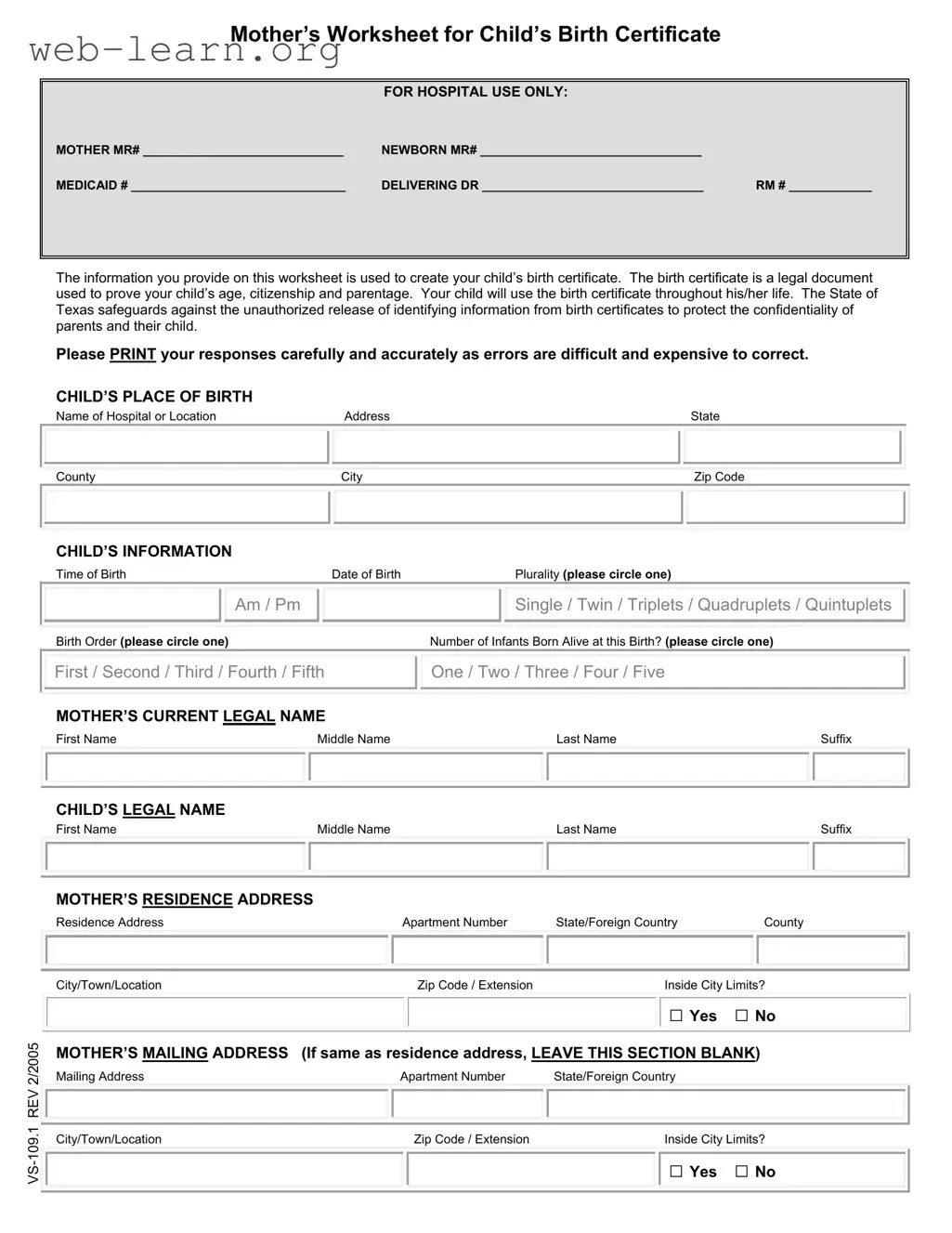
The Child Birth Certificate Texas form is an essential document for new parents, capturing vital information needed to establish a child's identity and legal status. This form includes a worksheet for the mother, designated for hospital use only, and requires details such as the mother’s and child’s names, birth dates, and places of birth. It also asks for the delivering doctor's information and the mother's residence and mailing addresses. Parents must provide comprehensive data regarding their education, occupation, and health information, including any Medicaid details, which can facilitate access to medical services for the child. The form emphasizes the importance of accuracy, as mistakes can lead to complications and costly corrections. Additionally, it outlines the process for obtaining a certified copy of the birth certificate and the child’s social security number, ensuring that parents understand the implications of the information they provide. The form also addresses paternity acknowledgment, marital status, and the mother's health during pregnancy, making it a critical component in documenting a child's birth in Texas.
| Fact Name | Description |
|---|---|
| Purpose of the Birth Certificate | The birth certificate serves as a legal document that proves a child's age, citizenship, and parentage. It is essential for various life activities, such as enrolling in school and applying for government services. |
| Confidentiality Protection | Texas law safeguards against the unauthorized release of identifying information from birth certificates, ensuring the confidentiality of parents and their child. |
| Information Accuracy | Providing accurate information is crucial. Errors on the birth certificate can be difficult and costly to correct, making careful completion of the form necessary. |
| Social Security Application | If the mother indicates she wants to apply for the baby’s Social Security number, the birth information will be forwarded to the Social Security Administration for processing. |
| Medicaid Information | Completion of the Medicaid section allows for the newborn's Medicaid information to be processed and sent to the relevant authorities, typically taking 4-6 weeks. |
| Governing Laws | The Texas Health and Safety Code, specifically HSC §192.003, governs the reporting of birth data and the creation of birth certificates in Texas. |
Completing the Child Birth Certificate form in Texas is essential for establishing your child's identity and legal status. This document will be used throughout your child's life for various purposes, including school enrollment and applying for government services. Ensure that you fill out the form accurately, as mistakes can be challenging to rectify.
After completing the form, submit it to the hospital staff. They will use this information to prepare your child's official birth certificate. Ensure that you keep a copy of the completed form for your records. If you have any questions or need assistance, don't hesitate to ask the hospital staff for help.
How do I get a copy of my baby’s birth certificate?
You can request and purchase a certified copy of your child’s birth certificate from the local registrar’s office in the city or county where the birth occurred. Alternatively, you can obtain it from the Texas Vital Statistics office located in Austin, Texas. A certified birth certificate is a permanent legal document that establishes your child's identity and is essential for applying for medical or government services, passports, school admissions, and more.
When will I receive my baby’s social security card?
If you indicated "Yes" to the question about applying for your baby’s social security number, the birth information will be sent to the Social Security Administration as soon as the Texas Vital Statistics office receives it from the hospital. The Social Security Administration typically takes 2-3 weeks to process the information. Expect the social security card to be mailed to the mother’s provided mailing address. The entire process usually takes about 4-6 weeks to complete.
When will I receive my baby’s Medicaid number?
If you filled out the questions regarding the mother’s Medicaid name and number, the birth information will also be forwarded to the Medicaid office once the Texas Vital Statistics office has the data from the hospital. Medicaid generally requires 2-3 weeks for processing. An Infant Medicaid card will be sent to the mother’s mailing address, and the entire process usually takes around 4-6 weeks.
What information is required on the Child Birth Certificate Texas form?
The form requires various details, including:
Accurate and careful completion of this form is crucial, as errors can be challenging and costly to correct.
What happens if I make a mistake on the birth certificate form?
Errors on the birth certificate form can lead to complications later in life, such as issues with identity verification or access to services. If a mistake occurs, it may require a formal correction process, which can be both time-consuming and expensive. Therefore, it is essential to double-check all entries before submission.
Can the father's name be included on the birth certificate if the parents are not married?
Yes, the father's name can be included on the birth certificate if both parents complete an Acknowledgment of Paternity. If the mother has been married to someone other than the biological father within 300 days before the child’s birth, a Denial of Paternity from the husband or former husband is also required to include the biological father's information.
What is the importance of the birth certificate?
A birth certificate is a fundamental legal document that proves a child's age, citizenship, and parentage. It is often required for various purposes, including applying for a passport, enrolling in school, and accessing medical services. Having a certified copy readily available is crucial for navigating many aspects of life.
When filling out the Child Birth Certificate Texas form, many parents inadvertently make mistakes that can complicate the process of obtaining an accurate birth certificate. Here are ten common errors to avoid.
One frequent mistake is not providing complete information about the child's place of birth. Parents sometimes forget to include the full name of the hospital or location, along with the correct address and zip code. This information is crucial, as it helps establish the legal birthplace of the child.
Another common error involves the child's name. Parents may miswrite the child's legal name, including the first, middle, and last names. It’s essential to double-check the spelling and ensure that all parts of the name are included, especially any suffixes like Jr. or III.
Many people overlook the importance of accurately indicating the time and date of birth. Mistakes in this section can lead to complications later when trying to verify age or citizenship. It is best to confirm these details with hospital records before submitting the form.
In some cases, parents may forget to circle the correct plurality and birth order. This is particularly important for multiple births, as it helps clarify the specific details of the delivery. Parents should take extra care to ensure these sections are filled out correctly.
Parents often neglect to provide the mother's current legal name accurately. This includes the first, middle, last names, and any suffixes. Failing to do so can create confusion and may lead to issues when trying to obtain legal documents in the future.
Another mistake is not specifying the mother's residence address correctly. Parents should include all necessary details, such as the apartment number, city, and zip code. Incomplete addresses can delay the processing of the birth certificate.
Some parents do not fill out the mother's education and occupation sections. While this information may seem trivial, it is required for statistical purposes. Omitting this can lead to unnecessary delays.
When it comes to the father's information, many parents either leave it blank or provide incorrect details. If the father is to be included on the birth certificate, both parents must complete an Acknowledgment of Paternity. Not following this procedure can complicate matters later on.
Another oversight involves the mother's marital status. Parents may not read the instructions carefully, leading to incorrect selections. This can affect the father's rights and responsibilities concerning the child.
Finally, many parents forget to consent to the inclusion of their baby's immunization information in the statewide Immunization Registry. This is an important step for future healthcare needs and should not be overlooked.
By being mindful of these common mistakes, parents can ensure a smoother process when filling out the Child Birth Certificate Texas form. Taking the time to review each section carefully can save time and prevent complications down the line.
In addition to the Child Birth Certificate Texas form, several other forms and documents are often required or recommended for new parents. Each of these documents serves a specific purpose in the process of registering a child's birth and ensuring the appropriate legal and medical information is captured.
These documents collectively support the legal and medical framework surrounding a child's birth. Ensuring that each form is accurately completed and submitted can help prevent future complications regarding identity, citizenship, and healthcare access.
Filling out the Texas Child Birth Certificate form is a crucial task that requires attention to detail. To ensure accuracy and efficiency, here are some important dos and don'ts to keep in mind:
Completing this form accurately will ensure that your child's birth certificate is processed without unnecessary complications. Remember, this document is essential for your child's identity and future needs.
Understanding the Child Birth Certificate Texas form is essential for new parents. However, several misconceptions can lead to confusion. Below are four common misconceptions about this form, along with clarifications.
While the birth certificate is indeed a legal document, it serves multiple functions. It proves your child's age, citizenship, and parentage, which are necessary for various activities throughout their life, such as enrolling in school and applying for government services.
Errors on the Child Birth Certificate Texas form can be difficult and costly to correct. It is crucial to provide accurate information when filling out the form to avoid complications later.
For unmarried parents, the father's name can only be included on the birth certificate if both parents complete an Acknowledgment of Paternity. If the mother has been married to someone other than the biological father within 300 days prior to the birth, additional documentation is required.
While parents can apply for a Social Security number for their child through the birth certificate form, the processing of the Social Security card occurs separately. It typically takes 4-6 weeks for the card to arrive after the birth information is submitted to the Social Security Administration.
Filling out the Texas Child Birth Certificate form is an important step for new parents. Here are key takeaways to ensure the process goes smoothly: