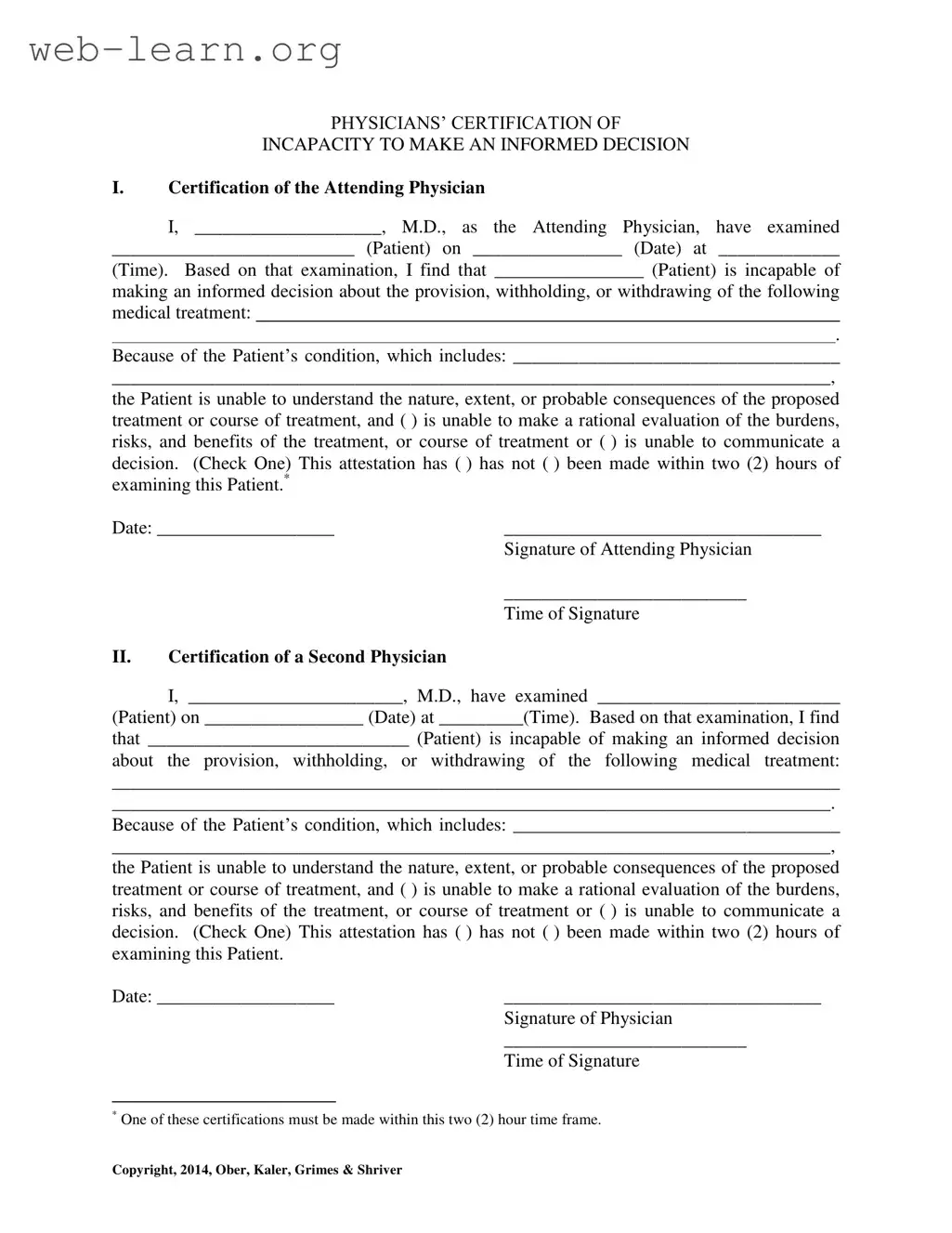
When navigating the complexities of healthcare decisions, understanding the Certification of Incapacity form is essential. This document serves a critical role in determining whether a patient is capable of making informed choices regarding their medical treatment. It requires the assessment of two physicians who must evaluate the patient's ability to comprehend the nature and consequences of proposed treatments. The form includes sections for both the attending physician and a second physician to certify their findings, ensuring a thorough evaluation. Key details such as the patient's condition and the specific treatments being considered must be documented. Additionally, the physicians must indicate whether the patient is unable to make rational decisions or communicate their choices. Timeliness is crucial; one of the certifications must be completed within two hours of the examination. This structure not only protects the rights of patients but also provides clarity and support for families and caregivers during challenging times.

| Fact Name | Description |
|---|---|
| Purpose | The Certification of Incapacity form is used to determine a patient's ability to make informed medical decisions. |
| Attending Physician Requirement | The form must be completed by the attending physician who has examined the patient. |
| Second Physician Certification | A second physician must also certify the patient's incapacity, ensuring an additional layer of verification. |
| Time Frame | Both certifications must be made within two hours of the examination to be valid. |
| Patient's Condition | The form requires a detailed description of the patient's condition that affects their decision-making ability. |
| State-Specific Laws | Governed by state-specific laws, such as the Uniform Health-Care Decisions Act, which varies by jurisdiction. |
Completing the Certification of Incapacity form requires careful attention to detail. This form is essential for documenting a patient's inability to make informed medical decisions. Following these steps will help ensure that the form is filled out correctly.
Next, proceed to the Certification of a Second Physician section. Repeat similar steps for the second physician, ensuring all required information is accurately filled out.
What is the purpose of the Certification of Incapacity form?
The Certification of Incapacity form serves to document that a patient is unable to make informed medical decisions due to their current health condition. This form is typically completed by attending physicians and may require a second physician's certification. It ensures that medical professionals have a clear understanding of the patient's capacity to consent to or refuse treatment, which is essential for making ethical and legal medical decisions.
Who can complete the Certification of Incapacity form?
Only licensed medical doctors (M.D.s) can complete this form. The attending physician, who has examined the patient, is responsible for the first certification. A second physician must also evaluate the patient and provide their own certification. This dual certification process helps to ensure accuracy and provides a safeguard for patients who may be vulnerable due to their medical condition.
What criteria must be met for a patient to be considered incapacitated?
A patient is deemed incapable of making informed decisions if they cannot understand the nature, extent, or probable consequences of the proposed medical treatment. Additionally, they may be unable to evaluate the risks and benefits of the treatment rationally or communicate a decision effectively. Physicians must check one of these criteria on the form to confirm the patient's incapacity.
What is the significance of the two-hour time frame mentioned in the form?
The two-hour time frame is crucial because it ensures that the assessments of the patient’s incapacity are timely and relevant. One of the physicians must complete their certification within this period following their examination of the patient. This requirement helps to maintain the integrity of the decision-making process and ensures that the patient's condition has not changed significantly during that time.
Filling out the Certification of Incapacity form is an important task that can have significant implications for a patient’s care. However, many individuals make common mistakes that can lead to complications. One frequent error is failing to provide complete patient information. It is crucial to fill in the patient's name, date, and time of the examination accurately. Missing or incorrect details can create confusion and delay necessary medical decisions.
Another mistake often seen is neglecting to check the appropriate box regarding the patient’s ability to make a decision. The form requires a clear indication of whether the patient can evaluate the burdens, risks, and benefits of treatment or if they can communicate a decision. Omitting this step can result in misunderstandings about the patient’s capacity and may affect their treatment options.
In addition, some individuals overlook the importance of the timing of the certification. The form specifies that one of the certifications must be made within two hours of the examination. If this time frame is not adhered to, the validity of the certification may be questioned, potentially impacting the patient’s care. It is essential to be mindful of this requirement to ensure that the certification holds up under scrutiny.
Furthermore, the signatures of the attending physician and the second physician must be included. Failing to obtain both signatures can render the form incomplete. This oversight can lead to delays in treatment and may require additional steps to rectify the situation, adding stress to an already challenging time for the patient and their loved ones.
Lastly, individuals sometimes do not provide a thorough explanation of the patient's condition. The section detailing the patient’s condition should be filled out with care. A vague or incomplete description may not accurately reflect the patient's incapacity and could lead to inappropriate medical decisions. Clear and comprehensive information is vital for ensuring that the patient receives the best possible care.
The Certification of Incapacity form is an important document used in healthcare settings to establish a patient's ability to make informed decisions regarding their medical treatment. Alongside this form, several other documents may be necessary to ensure comprehensive care and legal compliance. Below is a list of these additional forms and documents, each serving a specific purpose.
Each of these documents plays a crucial role in the overall healthcare process, particularly when a patient is unable to make decisions for themselves. It is essential for caregivers and family members to understand these forms to ensure that a patient's rights and preferences are respected at all times.
The Certification of Incapacity form shares similarities with several other important legal documents. Each serves a specific purpose related to medical decision-making and patient rights. Below is a list of six documents that are comparable to the Certification of Incapacity form:
When filling out the Certification of Incapacity form, it's important to follow specific guidelines to ensure accuracy and compliance. Here are six things to keep in mind:
By following these guidelines, you can help ensure that the Certification of Incapacity form is filled out correctly and effectively supports the patient's needs.
Understanding the Certification of Incapacity form is essential for both patients and their families. However, several misconceptions can lead to confusion. Here are four common misconceptions:
Addressing these misconceptions can help ensure that patients receive the appropriate care and that their rights and preferences are respected.
Filling out the Certification of Incapacity form is an important process for ensuring that patients receive appropriate medical care when they cannot make informed decisions. Here are key takeaways to consider: