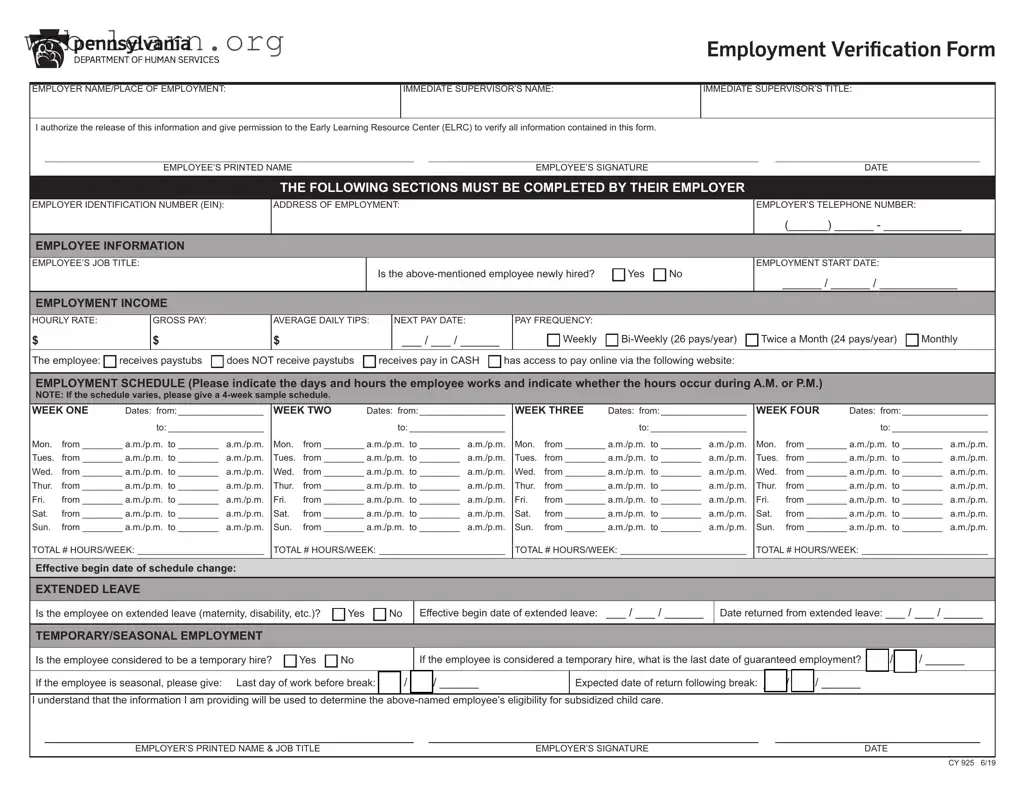
The Ccis Employment Verification Form serves a crucial role in the process of verifying an employee's work status and income, particularly for those seeking assistance with child care costs. This form requires detailed information from both the employee and their employer. Employers must provide their identification number, address, and contact details, along with specific information about the employee's job title, start date, and income. The form also captures the employee's work schedule, detailing hours worked each day and whether those hours fall in the A.M. or P.M. Additionally, it addresses the employee's status regarding pay frequency and whether they receive paystubs. For employees on extended leave or those with temporary or seasonal employment, the form includes sections to note these circumstances. Completing this form accurately is vital, as it directly impacts the employee's eligibility for subsidized child care programs. Employers are reminded to submit the completed form directly to the Early Learning Resource Center (ELRC), ensuring that an authorized representative, not the employee, fills it out. This verification process not only supports employees but also fosters a smoother experience for families seeking essential child care assistance.
| Fact Name | Description |
|---|---|
| Purpose of the Form | The Ccis Employment Verification Form is used to confirm an employee's job status and income for subsidized child care eligibility. It is essential for employees seeking assistance with child care costs. |
| Required Information | Employers must provide specific details, including the employee's job title, income, work schedule, and whether the employee is newly hired. This information helps in assessing eligibility for financial assistance. |
| Completion Responsibility | The form must be completed by an authorized company representative, not the employee. This ensures that the information provided is accurate and verified by someone in a position of authority. |
| Governing Law | This form is governed by state laws related to child care assistance programs, which vary by state. For example, in Pennsylvania, it falls under the Child Care Development Block Grant regulations. |
To complete the CCIS Employment Verification form, follow these steps carefully. This form is essential for verifying employment details for employees seeking assistance with child care costs. Accurate information will ensure that the verification process runs smoothly.
What is the purpose of the CCIS Employment Verification Form?
The CCIS Employment Verification Form is designed to verify an employee's employment status and income. This verification is crucial for determining eligibility for subsidized child care programs. The form must be completed by an authorized representative of the employer, not the employee themselves.
Who is responsible for completing the form?
An authorized company representative must fill out the form. This person should have access to accurate information regarding the employee’s job title, income, and work schedule. The employee cannot complete the form themselves, as it requires verification from the employer.
What specific information is required from the employer?
The employer must provide several key pieces of information, including:
What if the employee’s work schedule varies?
If the employee’s work schedule changes from week to week, the employer must provide a sample schedule for four weeks. This schedule should specify the days and hours worked, clearly indicating whether the hours are in the A.M. or P.M.
How is the information used?
The information provided on the form is used to assess the employee’s eligibility for subsidized child care. Accurate details regarding employment status and income are essential for this evaluation.
Is the employee’s consent required for this verification?
Yes, the employee must authorize the release of their employment information. This consent is typically indicated by the employee’s signature on the form, allowing the Early Learning Resource Center (ELRC) to verify the details provided.
What should be done if the employee is on extended leave?
If the employee is on extended leave, the employer must indicate this on the form. The employer should provide the effective date of the leave and the expected return date. This information is important for understanding the employee's current employment status.
How should the completed form be submitted?
The completed form must be mailed directly to the Early Learning Resource Center (ELRC). It is important to ensure that the form is sent promptly to avoid delays in processing the employee’s eligibility for child care assistance.
What if there are questions about completing the form?
If there are any questions or uncertainties regarding how to fill out the form, employers can contact the ELRC directly. The contact information is provided on the form, ensuring that assistance is readily available.
Filling out the CCIS Employment Verification form can seem straightforward, but there are common mistakes that can lead to delays or complications. Here are seven mistakes to watch out for when completing this important document.
First, many people forget to include the Employer Identification Number (EIN). This number is crucial for verifying the employer's identity. Without it, the form may be deemed incomplete. Make sure to double-check that this information is accurately provided.
Another frequent error is leaving the employee’s job title blank. This detail is essential for understanding the employee's role within the company. If this section is not filled out, it can cause unnecessary back-and-forth communication with the Early Learning Resource Center.
Additionally, some employers do not specify whether the employee is newly hired. This simple yes or no answer can significantly impact the verification process. Be sure to answer this question clearly to avoid confusion.
When it comes to the employment schedule, many people fail to indicate whether the hours are in A.M. or P.M. This oversight can lead to misunderstandings about the employee's working hours. Always clarify the time format to ensure accuracy.
Another common mistake is not providing a complete four-week sample schedule when the employee's hours vary. If the schedule changes from week to week, this information is vital for the verification process. Failing to include this can result in delays.
Some employers also overlook the section regarding extended leave. If an employee is on maternity or disability leave, this must be noted. Leaving this section blank can lead to complications in the verification of the employee’s eligibility for subsidized child care.
Finally, ensure that the form is signed by an authorized company representative. Many people mistakenly think that the employee can sign it. This is not the case. The form must be completed and signed by someone in a position of authority within the company.
By avoiding these common mistakes, you can help ensure that the CCIS Employment Verification form is completed accurately and efficiently, paving the way for a smoother verification process.
When navigating the employment verification process, especially in relation to child care subsidies, several key documents often accompany the CCIS Employment Verification Form. These documents provide additional context and information about the employee's work situation, ensuring that all necessary details are accurately captured. Below is a list of commonly used forms and documents that complement the employment verification process.
Collectively, these documents play a crucial role in the employment verification process. They help ensure that all information is accurate and comprehensive, ultimately supporting the employee's eligibility for child care assistance. By understanding the purpose of each document, both employers and employees can navigate this process more effectively.
When filling out the CCIS Employment Verification form, it’s essential to ensure accuracy and clarity. Here are some dos and don’ts to keep in mind:
Understanding the Ccis Employment Verification form is essential for both employers and employees. However, several misconceptions can lead to confusion. Here are six common misconceptions:
Addressing these misconceptions can help streamline the process and ensure that employees receive the assistance they need for child care costs.
Filling out the CCIS Employment Verification form is an important step in assisting employees with their child care costs. Here are key takeaways to keep in mind:
By following these guidelines, you can help facilitate the process for employees seeking child care assistance. Your attention to detail and commitment to accuracy make a significant difference.