The Caregiver Daily Log form serves as an essential tool for documenting the services provided by caregivers to their clients. This form captures vital information such as the caregiver's name, the policy number, and the claimant's name, ensuring that all parties involved have a clear record of care. It requires caregivers to check the location of service, whether it be at home or in a facility, and to identify their qualifications, such as Certified Home Health Aide or RN. Each visit necessitates the completion of this form in ink, with caregivers instructed to retain a copy for their records. The log includes a detailed breakdown of services rendered, including assistance with bathing, dressing, and toileting, as well as supervision for clients with cognitive impairments. Caregivers must document the date of service, arrival and departure times, total hours worked, and the corresponding charges. A section also inquires whether the client was hospitalized during the week, which is critical for processing claims. Both the caregiver and the claimant or legal representative must sign the form to certify that the information is accurate and complete, underscoring the importance of honesty in the caregiving process. Lastly, a fraud notice alerts users to the serious implications of submitting false information, reinforcing the integrity of the claims process.

| Fact Name | Details |
|---|---|
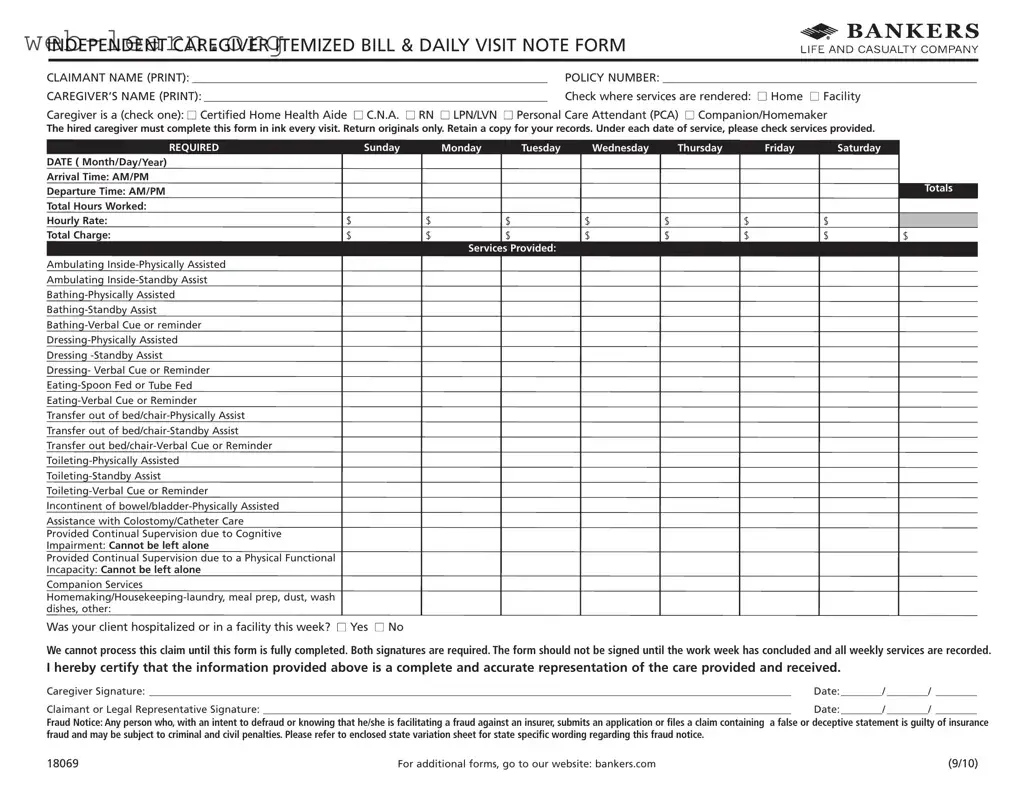
| Purpose of the Form | The Caregiver Daily Log form is designed to document the services provided by caregivers to clients, ensuring accurate billing and care tracking. |
| Required Signatures | Both the caregiver and the claimant or legal representative must sign the form. This requirement ensures accountability and verifies that the information is accurate. |
| Services Documentation | Caregivers must check off the specific services provided during each visit. This detailed documentation helps in assessing the care delivered and in processing claims. |
| Completion Guidelines | The form must be completed in ink and returned as an original. Caregivers are advised to retain a copy for their records, which is crucial for personal documentation. |
| Fraud Notice | The form includes a fraud notice, warning that submitting false information can lead to criminal and civil penalties. This notice serves to protect both insurers and caregivers. |
Completing the Caregiver Daily Log form accurately is essential for ensuring that all services provided are documented and that claims can be processed smoothly. Follow the steps outlined below to fill out the form correctly.
Once completed, retain a copy for your records and return the original form as instructed. This ensures that all details are accurately documented for processing claims.
What is the purpose of the Caregiver Daily Log form?
The Caregiver Daily Log form is designed to document the services provided by caregivers to individuals receiving care. It serves as an official record of the caregiver's activities during each visit, including the types of services rendered, the time spent, and the total charges incurred. This form is essential for ensuring accurate billing and for maintaining transparency between caregivers, clients, and insurance providers.
Who is required to complete the Caregiver Daily Log form?
The caregiver hired to provide services must complete the Caregiver Daily Log form. This includes a variety of professionals, such as Certified Home Health Aides, CNAs, RNs, LPNs/LVNs, Personal Care Attendants, and Companions/Homemakers. Each caregiver is responsible for accurately filling out the form in ink after every visit to ensure that all relevant details are captured.
What information needs to be included on the form?
The Caregiver Daily Log form requires several key pieces of information:
Completing all sections of the form is crucial for processing claims accurately and efficiently.
What happens if the form is not completed correctly?
If the Caregiver Daily Log form is not filled out completely or accurately, it may delay the processing of claims. Insurance providers require that all sections are properly completed before they can approve any reimbursements. Incomplete forms can lead to additional requests for information, which can prolong the payment process. Therefore, it is vital for caregivers to double-check their entries and ensure that both signatures are present before submitting the form.
Completing the Caregiver Daily Log form accurately is essential for ensuring proper processing of claims. However, several common mistakes can lead to delays or denials. Awareness of these errors can help caregivers submit a complete and correct form.
One frequent mistake is failing to fill out the claimant name and policy number sections. These details are crucial for identifying the client and verifying coverage. Omitting this information can result in significant delays in processing the claim.
Another common error is not signing the form. Both the caregiver and the claimant or legal representative must sign the document. Without these signatures, the form is incomplete and cannot be processed. Caregivers should ensure that signatures are obtained only after all services for the week have been recorded.
Inaccurate recording of service dates is also a prevalent mistake. Each date of service must be clearly indicated in the required format (Month/Day/Year). Errors in this section can lead to confusion regarding the days services were provided.
Caregivers often overlook the arrival and departure times. These times must be documented accurately to calculate total hours worked. If this information is missing or incorrect, it can affect the total charge and cause issues with payment.
Another mistake is not checking the appropriate services provided. Each service rendered during the visit should be marked clearly. Failing to do so can lead to underreporting of care provided, which may impact reimbursement.
Caregivers sometimes forget to include the hourly rate and total charge. This information is necessary for calculating the payment due. Without it, the claim may be rejected or delayed.
Another error occurs when caregivers do not retain a copy of the completed form. Keeping a copy is essential for record-keeping and can be helpful if questions arise about the claim later.
Additionally, caregivers may neglect to indicate whether the client was hospitalized or in a facility during the week. This information is important for the insurance company to understand the context of the care provided.
Lastly, caregivers sometimes submit the form without reviewing it for accuracy. Taking a moment to double-check all entries can prevent mistakes that may lead to delays or denials. Thoroughness is key to ensuring a smooth claims process.
The Caregiver Daily Log form is essential for documenting the services provided by caregivers. However, several other forms and documents may accompany it to ensure a comprehensive record of care. Below is a list of these related documents, each serving a specific purpose in the caregiving process.
These documents work together to create a clear picture of the caregiving process, ensuring that all parties involved have a thorough understanding of the services provided and the needs of the client. Keeping accurate records is crucial for effective communication and quality care.
The Caregiver Daily Log form serves a specific purpose in documenting the services provided by caregivers. However, there are several other documents that share similar characteristics in terms of structure and function. Here are seven documents that are comparable:
When filling out the Caregiver Daily Log form, attention to detail is crucial. Here are five important do's and don'ts to keep in mind:
Misconceptions about the Caregiver Daily Log form can lead to confusion and potential issues in processing claims. Here are five common misunderstandings:
Understanding these misconceptions can help caregivers navigate the claims process more effectively, ensuring that they receive timely and accurate compensation for their services.
Filling out the Caregiver Daily Log form accurately is essential for ensuring that caregivers receive proper compensation for their services. Here are some key takeaways to consider:
By following these guidelines, caregivers can help ensure a smooth process for billing and reimbursement, ultimately supporting the well-being of those they care for.