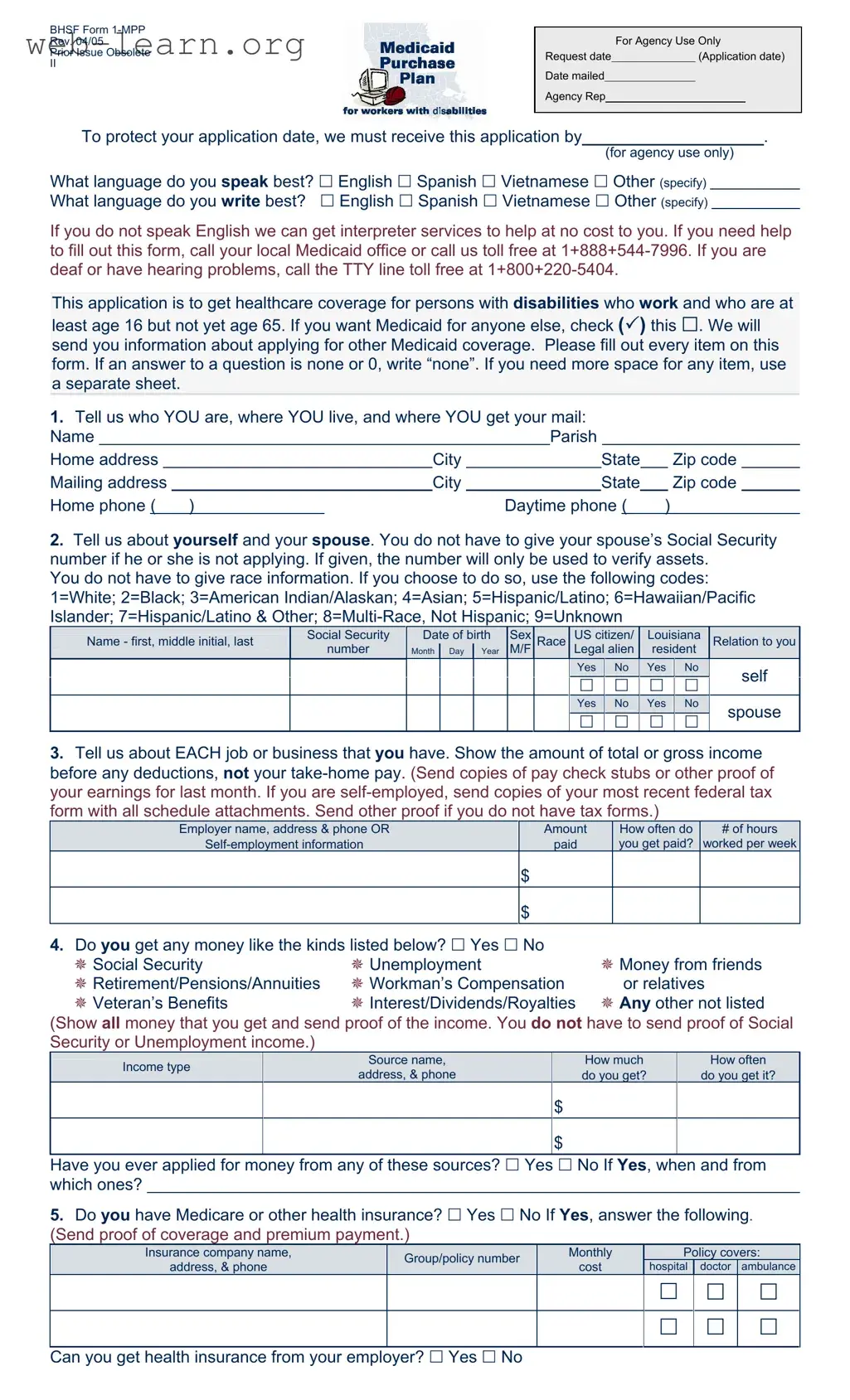
The Care 1St Arizona Prior Authorization form serves as a crucial tool for individuals seeking healthcare coverage under the Medicaid program, specifically designed for those with disabilities who are between the ages of 16 and 65. This form not only collects essential personal information, such as the applicant's name, address, and contact details, but also delves into their financial circumstances. Applicants are required to provide details about their income, assets, and any existing health insurance coverage. Furthermore, the form is structured to accommodate various languages, ensuring accessibility for non-English speakers through interpreter services. It emphasizes the importance of accuracy, urging applicants to fill out every section completely and truthfully, while also outlining the responsibilities associated with receiving Medicaid benefits. For those who may require assistance, guidance is readily available through local Medicaid offices and toll-free support lines. This comprehensive approach ensures that individuals can navigate the complexities of the application process with confidence and clarity.