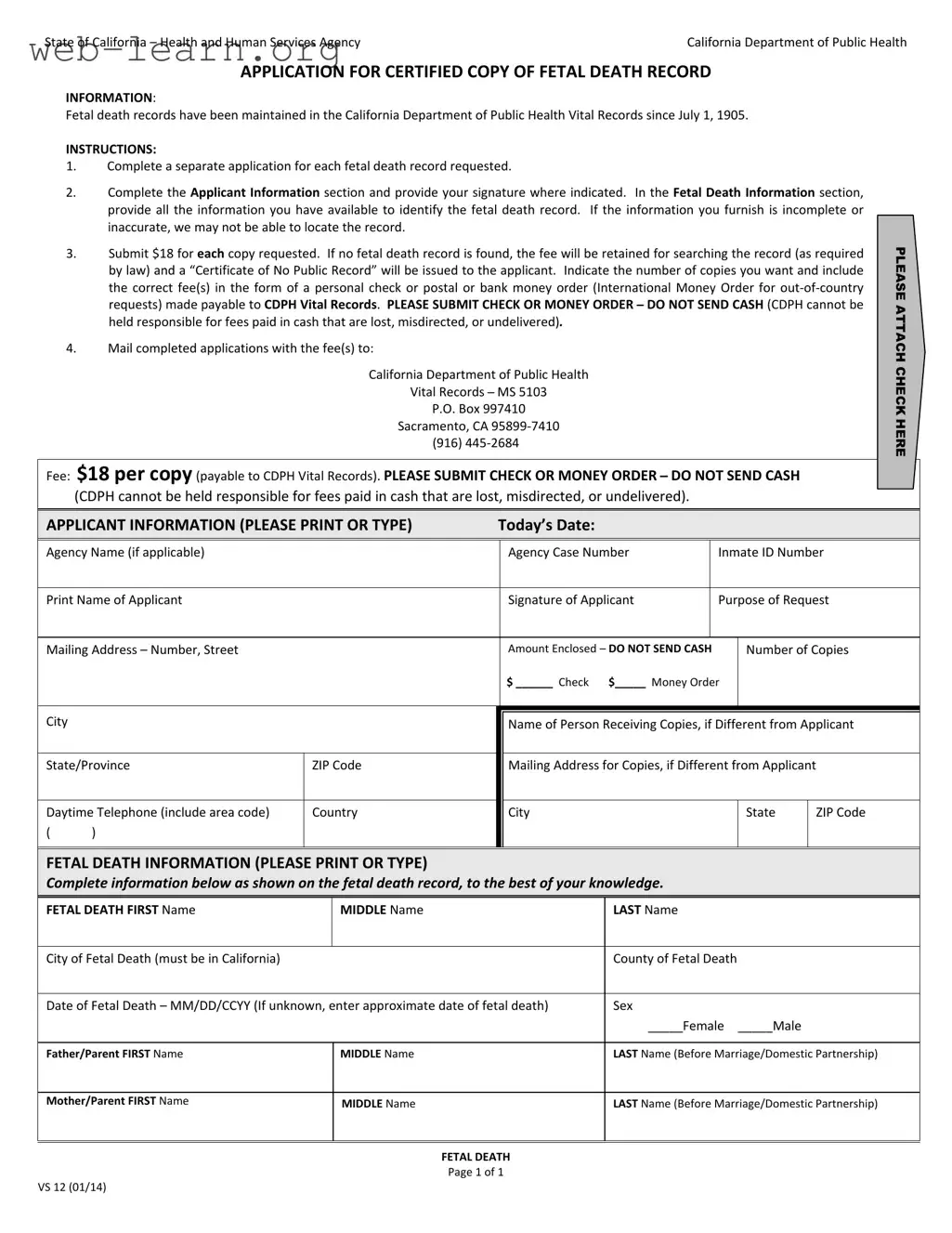
The California VS 12 form serves as a crucial document for those seeking certified copies of fetal death records in the state. Since July 1, 1905, the California Department of Public Health has maintained these vital records, providing families with a formal acknowledgment of their loss. To obtain a copy, applicants must complete a separate application for each fetal death record requested. The form requires detailed information, including the names of the parents, the date and location of the fetal death, and the applicant's contact information. Accuracy is essential; incomplete or incorrect information may hinder the ability to locate the desired record. Each request incurs a fee of $18, which covers the search and processing of the application. If no record is found, the fee is retained, and a "Certificate of No Public Record" will be issued. Payment must be made via check or money order, as cash is not accepted. Once completed, applications should be mailed to the specified address in Sacramento, ensuring that families can receive the documentation they need during such a sensitive time.
| Fact Name | Description |
|---|---|
| Governing Agency | The application is managed by the California Department of Public Health. |
| Record Maintenance | Fetal death records have been kept since July 1, 1905. |
| Application Requirement | A separate application is needed for each fetal death record requested. |
| Fee Structure | The fee for each copy is $18, payable by check or money order. |
| Fee Retention Policy | If no record is found, the fee is retained, and a “Certificate of No Public Record” is issued. |
| Mailing Instructions | Completed applications must be mailed to the California Department of Public Health, Vital Records. |
| Prohibited Payment Method | Cash payments are not accepted; only checks or money orders should be sent. |
After completing the California VS 12 form, you will submit it along with the required fee to obtain a certified copy of a fetal death record. Ensure that all information is accurate and complete to avoid any delays in processing your request.
What is the California VS 12 form?
The California VS 12 form is an application for obtaining a certified copy of a fetal death record. This form is managed by the California Department of Public Health and has been in use since July 1, 1905. It allows individuals to request official documentation regarding fetal deaths that occurred in California.
Who can apply for a fetal death record using this form?
Any individual who is directly related to the deceased or has a legitimate interest can apply for a fetal death record. This includes parents, legal guardians, or authorized representatives. It is important to provide the necessary information to establish your relationship or interest.
What information do I need to provide on the form?
You need to complete the Applicant Information section, which includes your name, address, and contact details. In the Fetal Death Information section, provide as much detail as possible about the fetal death, including:
Accurate information is crucial for locating the record.
How much does it cost to obtain a copy of a fetal death record?
The fee for each copy of a fetal death record is $18. This amount must be submitted with your application in the form of a personal check or a postal or bank money order. If no record is found, the fee will not be refunded, but a “Certificate of No Public Record” will be issued.
Where do I send my completed application?
You should mail your completed application, along with the payment, to the following address:
California Department of Public Health
Vital Records – MS 5103
P.O. Box 997410
Sacramento, CA 95899-7410
Can I pay the fee in cash?
No, you cannot pay the fee in cash. The California Department of Public Health does not accept cash payments. Payments must be made via check or money order to avoid the risk of loss or misdirection.
What should I do if I do not have all the required information?
If you do not have complete information, you should provide as much detail as you can. Incomplete or inaccurate information may hinder the ability to locate the fetal death record. It is better to include approximate dates or any known details rather than leaving sections blank.
What happens if the fetal death record is not found?
If the record is not found, the fee you paid will be retained for the search. You will receive a “Certificate of No Public Record” confirming that no record exists for the information you provided.
How can I check the status of my application?
Is there a way to expedite my request?
Currently, the California Department of Public Health does not offer an expedited service for fetal death record requests. Processing times may vary, so it is advisable to submit your application well in advance if you need the record by a specific date.
Filling out the California VS 12 form can be a straightforward process, but many people make common mistakes that can delay their requests. One frequent error is not completing a separate application for each fetal death record requested. It is essential to follow this instruction to ensure that each record is processed correctly.
Another mistake often made is failing to provide complete and accurate information in the Fetal Death Information section. Incomplete or inaccurate details can lead to difficulties in locating the record. Always double-check the information you provide to avoid unnecessary delays.
Many applicants also forget to sign the form in the designated area. A missing signature can result in the application being returned or rejected. It is vital to ensure that your signature is included before sending the form.
Some people overlook the payment instructions. The form requires a fee of $18 for each copy requested. If the payment is not included or is in the wrong form, such as cash, it can cause significant delays. Always use a personal check or money order made payable to CDPH Vital Records.
Another common mistake is not indicating the number of copies needed. This information is crucial for processing the request correctly. Be sure to specify how many copies you are requesting to avoid confusion.
Applicants sometimes forget to include their contact information. Providing a daytime telephone number and an accurate mailing address is essential. This allows the department to reach you if there are any issues with your application.
Some individuals also fail to attach their payment correctly. The instructions clearly state to "please attach check here." Not following this instruction can lead to the payment being lost or misdirected.
In addition, people often do not provide the correct mailing address for copies if it differs from the applicant's address. Ensure that this information is accurate to avoid delays in receiving the requested records.
Another mistake involves entering an incorrect date format for the fetal death. The form requires the date in MM/DD/CCYY format. Not adhering to this format can lead to processing issues.
Finally, applicants may neglect to verify the county and city of fetal death. This information must be accurate and must correspond to a location in California. Double-checking this detail can save time and prevent complications in locating the record.
The California VS 12 form is essential for individuals seeking a certified copy of a fetal death record. However, several other forms and documents may accompany this application to facilitate the process or provide additional information. Below is a list of relevant documents commonly used alongside the California VS 12 form.
Understanding these forms and documents can simplify the process of obtaining vital records in California. Each document serves a specific purpose, ensuring that applicants can effectively navigate the system and fulfill their needs.
The California VS 12 form, which is used to request a certified copy of a fetal death record, shares similarities with several other important documents in terms of purpose and structure. Below are four documents that are comparable to the California VS 12 form:
When filling out the California VS 12 form, it’s important to follow specific guidelines to ensure your application is processed smoothly. Here’s a helpful list of things you should and shouldn’t do:
By following these guidelines, you can help ensure that your application for a fetal death record is processed without unnecessary delays. Good luck!
Understanding the California VS 12 form can be challenging, and there are several misconceptions surrounding its use and requirements. Here are nine common misunderstandings, along with clarifications to help you navigate the process more effectively.
By understanding these misconceptions, applicants can better prepare themselves for the process of obtaining fetal death records in California, ensuring that they have all the necessary information and documentation ready for submission.
When filling out and using the California Vs 12 form for requesting a certified copy of a fetal death record, consider the following key takeaways: