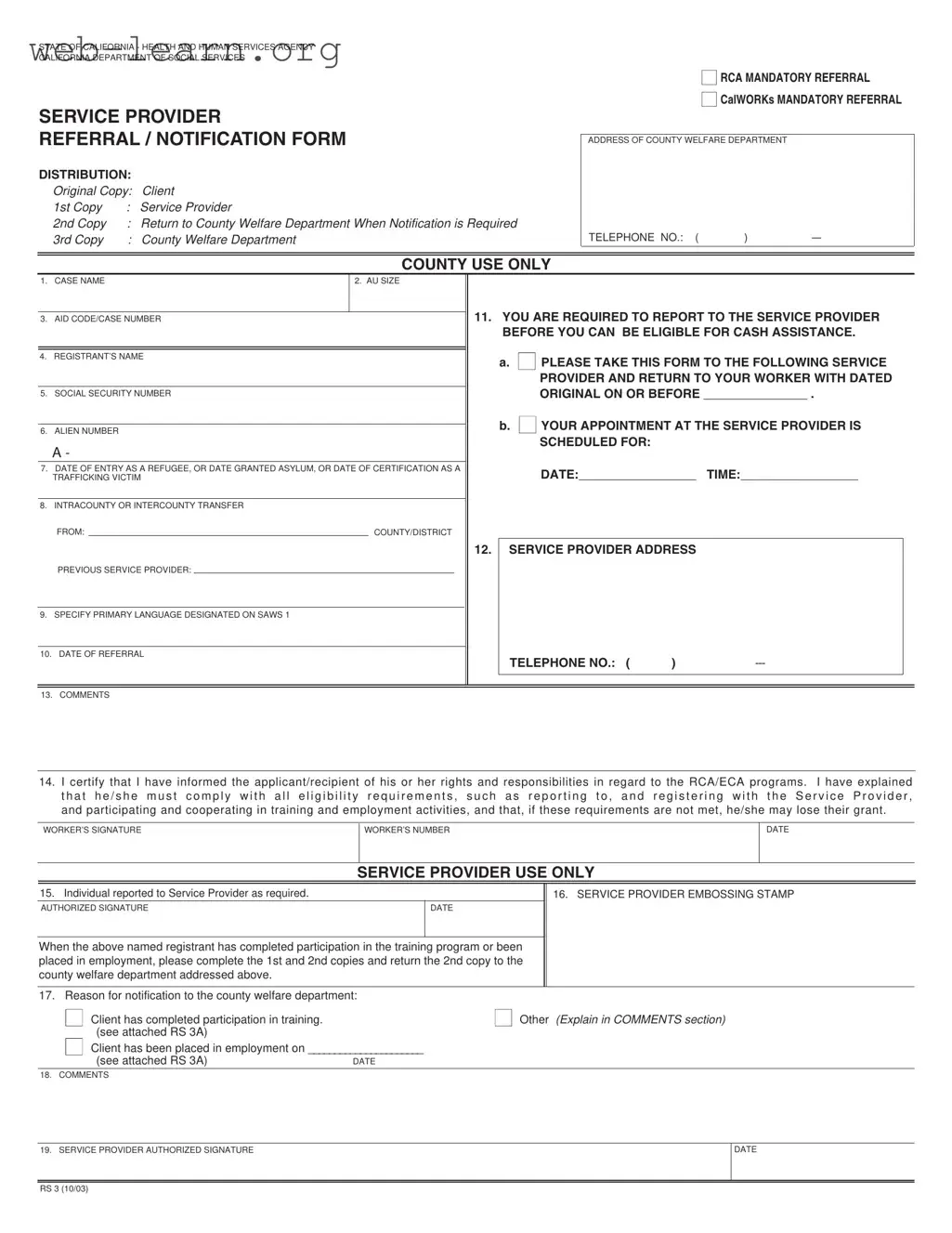
The California Rs 3 form plays a crucial role in the state's social services framework, particularly for individuals seeking assistance through programs like Refugee Cash Assistance (RCA) and CalWORKs. This mandatory referral form is designed to ensure that applicants comply with essential eligibility requirements before they can access cash assistance. It serves as a notification tool, detailing the steps that clients must take to connect with designated service providers. Key components of the form include the registrant's name, case number, and social security number, all of which help identify the individual within the assistance program. Additionally, the form outlines the responsibilities of the registrant, emphasizing the importance of attending scheduled appointments with service providers. By documenting these interactions, the Rs 3 form not only facilitates communication between clients and service providers but also helps maintain accountability within the welfare system. Moreover, it includes sections for comments and worker signatures, ensuring that all parties involved understand their roles and obligations. Ultimately, this form is an integral part of the process that supports individuals in navigating the complexities of social assistance in California.

| Fact Name | Description |
|---|---|
| Purpose | The California RS 3 form serves as a mandatory referral and notification tool for clients participating in the RCA and CalWORKs programs. |
| Distribution | The form has multiple copies: the original for the client, one for the service provider, and one for the county welfare department. |
| Eligibility Requirements | Clients must report to the designated service provider to remain eligible for cash assistance, as indicated on the form. |
| Governing Law | The RS 3 form is governed by California Welfare and Institutions Code, Sections 11200 and 11265. |
| Client Responsibilities | Clients must comply with all eligibility requirements, including registration with the service provider and participation in training and employment activities. |
| Service Provider Notification | The form requires service providers to notify the county welfare department when a client completes training or secures employment. |
Filling out the California RS 3 form requires careful attention to detail. Each section must be completed accurately to ensure proper processing. After you fill out the form, you will need to return it to the appropriate county welfare department. This step is crucial for maintaining eligibility for cash assistance.
What is the California RS 3 form?
The California RS 3 form is a notification and referral document used by the California Department of Social Services. It is primarily for individuals participating in the Refugee Cash Assistance (RCA) or Employment Cash Assistance (ECA) programs. This form ensures that clients report to designated service providers to maintain eligibility for cash assistance.
Who needs to complete the RS 3 form?
The form must be completed for individuals in the Assistance Unit (AU) who are required to register with a service provider. This includes refugees and individuals granted asylum or certification as trafficking victims.
What information is required on the RS 3 form?
Completing the form accurately is crucial for processing the referral and ensuring compliance with eligibility requirements.
What happens after the RS 3 form is completed?
Once the form is completed, the client must take it to the designated service provider. They are required to return the dated original to their caseworker by the specified deadline to maintain their eligibility for cash assistance.
What if the client misses their appointment?
If a client misses their appointment with the service provider, they may risk losing their cash assistance. It is essential to reschedule and report back to the caseworker as soon as possible.
How does the service provider verify attendance?
The service provider will sign and date the form to confirm that the client has reported for registration. This verification is critical for notifying the county welfare department about the client's compliance.
What is the purpose of the comments section on the RS 3 form?
The comments section allows for additional notes or explanations regarding the client's situation. This can include reasons for referral or any other relevant information that may assist in the processing of the case.
What should be done after the client completes their training or finds employment?
The service provider must complete the necessary sections of the RS 3 form and return the second copy to the county welfare department. This informs them of the client’s progress and ensures proper documentation of their employment or training completion.
Where can I obtain the RS 3 form?
The RS 3 form can typically be obtained from the county welfare department or the designated service provider. It may also be available online through the California Department of Social Services website.
Filling out the California RS 3 form is a critical step for those seeking assistance through the state’s programs. However, many individuals encounter pitfalls that can delay their application or lead to complications. Here are ten common mistakes to avoid when completing this important document.
One frequent error is failing to provide the correct case name. This should include the last name, first name, and middle initial of the refugee. A simple misspelling can cause confusion and delay processing. Always double-check this information to ensure accuracy.
Another common mistake is neglecting to specify the Aid Code/Case Number. This two-digit code is essential for identifying the appropriate public assistance program. Without it, the application may be misdirected or even rejected, leaving the applicant without necessary support.
Many people also forget to include the registrant's social security number. This number is crucial for verifying identity and eligibility. Omitting it can lead to significant delays, as additional steps will be needed to obtain this information later.
It is equally important to accurately enter the Date of Entry to the U.S. or the date granted asylum. This date should match the documentation provided, such as the I-94 form. Discrepancies can result in complications with eligibility verification.
Additionally, some applicants overlook the requirement to indicate whether the transfer is intracounty or intercounty. This information helps the county welfare department understand the registrant's previous service provider and ensures proper handling of the case.
Another mistake involves the appointment details. If an appointment is scheduled with the service provider, it is essential to provide the correct date and time. Failing to do so can lead to missed appointments, which may jeopardize eligibility for assistance.
When it comes to the service provider address, applicants sometimes provide incomplete or inaccurate information. It is crucial to include the full address, including street number, city, and zip code. Missing details can lead to confusion and delays in processing.
In the comments section, some individuals provide vague or unclear information. This area is an opportunity to clarify any special circumstances or additional details that may assist the service provider. Clear communication can help facilitate a smoother process.
Finally, neglecting to obtain the authorized signature from the service provider can halt the entire process. This signature is necessary to confirm that the registrant has reported as required. Always ensure that this step is completed before submitting the form.
Avoiding these common mistakes can significantly improve the chances of a successful application. Attention to detail and thoroughness in filling out the California RS 3 form will help ensure that individuals receive the assistance they need without unnecessary delays.
The California Rs 3 form is an essential document used in the state's public assistance programs, particularly for refugees and asylees. Along with this form, there are several other documents that may be required during the process. Each of these forms serves a specific purpose and helps ensure that individuals receive the assistance they need. Below is a list of related forms commonly used in conjunction with the California Rs 3 form.
Understanding these forms can help streamline the process of obtaining assistance and ensure compliance with program requirements. Each document plays a vital role in supporting individuals as they navigate the public assistance system in California.
The California RS 3 form is a crucial document used in the context of public assistance programs. It shares similarities with several other forms that serve related purposes. Here are seven documents that are similar to the RS 3 form:
Each of these documents plays a vital role in ensuring that clients are aware of their obligations and the services available to them. Understanding these similarities can help clients navigate the assistance process more effectively.
When filling out the California RS 3 form, it is important to follow certain guidelines to ensure accuracy and compliance. Below is a list of things you should and shouldn't do.
Following these guidelines will help facilitate the processing of the RS 3 form and ensure that all necessary information is accurately reported.
Understanding the California Rs 3 form is crucial for those navigating the welfare system. However, several misconceptions can lead to confusion. Here are five common misconceptions:
It is essential for clients to fully understand their responsibilities related to the Rs 3 form. Misunderstandings can lead to delays in assistance or even loss of benefits. Staying informed and compliant is key to a successful experience with the welfare system.
Filling out and using the California Rs 3 form is an important process for individuals seeking assistance. Here are some key takeaways to keep in mind:
By following these key points, individuals can navigate the process more smoothly and ensure compliance with the requirements set forth by the California Department of Social Services.