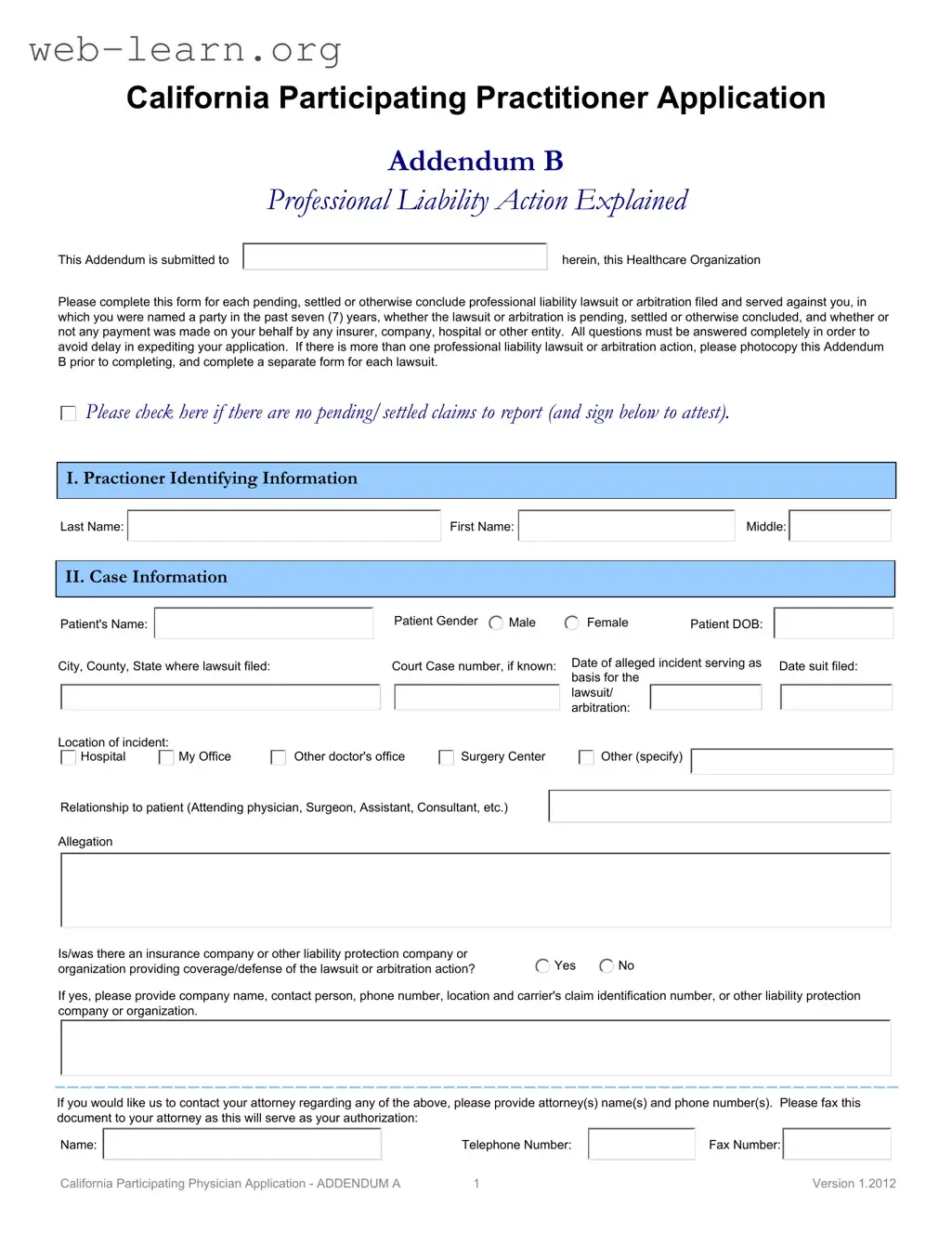
The California Participating Practitioner form is a crucial document for healthcare professionals seeking to participate in various healthcare organizations within the state. This form requires practitioners to disclose their professional liability history, specifically any pending or concluded lawsuits or arbitrations from the past seven years. Each practitioner must provide detailed information about the case, including the patient's name, the location of the incident, and the nature of the allegations. If multiple cases exist, practitioners should photocopy the form to ensure each one is documented separately. Additionally, the form includes sections to identify the practitioner and to summarize the circumstances surrounding each case. It emphasizes the importance of complete and accurate responses to avoid delays in the application process. By signing the form, practitioners also authorize the release of their malpractice insurance coverage and claims history, ensuring confidentiality while facilitating the credentialing process. This thorough approach helps healthcare organizations assess the qualifications and risk factors associated with each practitioner, ultimately promoting patient safety and quality care.
| Fact Name | Description |
|---|---|
| Purpose of Form | The California Participating Practitioner form is used to collect information about professional liability lawsuits or arbitrations involving healthcare practitioners. |
| Time Frame | Practitioners must report any lawsuits or arbitrations filed against them within the past seven years. |
| Multiple Actions | If there are multiple lawsuits or arbitrations, practitioners should photocopy the form and complete a separate addendum for each case. |
| Insurance Information | Practitioners must disclose whether there was any insurance or liability protection involved in the lawsuits or arbitrations. |
| Confidentiality Assurance | The information provided will be kept confidential and shared only for legitimate credentialing and peer review activities. |
| Governing Law | This form is governed by California law, specifically related to healthcare and professional liability regulations. |
| Applicant Signature | The form requires a signature from the applicant, and a stamp is not acceptable. |
| Attestation | Applicants must attest that the information provided is true and correct, ensuring accountability in the application process. |
Completing the California Participating Practitioner form requires careful attention to detail. After you fill out this form, it will be submitted to the healthcare organization for review. Make sure all sections are completed accurately to avoid any delays in processing your application.
What is the purpose of the California Participating Practitioner form?
The California Participating Practitioner form is designed to collect essential information regarding a practitioner's professional liability history. It aims to ensure that healthcare organizations can evaluate the qualifications and background of practitioners applying for participation in their networks. By gathering detailed information about any lawsuits or arbitration actions, the form helps maintain high standards of care and accountability within the healthcare system.
What information must be provided about professional liability lawsuits?
When completing the form, practitioners must disclose any pending, settled, or concluded professional liability lawsuits or arbitration actions from the past seven years. Specific details required include:
Practitioners must answer all questions completely to avoid delays in processing their application.
What should I do if I have multiple lawsuits to report?
If you have more than one professional liability lawsuit or arbitration action, it is necessary to photocopy Addendum B. Complete a separate form for each lawsuit to ensure that all relevant details are captured accurately. This practice helps maintain clarity and organization in the application process.
How do I certify the information provided in the form?
At the end of the form, practitioners are required to certify that the information they have provided is true and correct. This certification is an important step, as it affirms the accuracy of the details shared and the practitioner's commitment to transparency. Signing the form also grants permission for the healthcare organization to verify the information, ensuring that it is used solely for legitimate credentialing and peer review purposes.
What if there are no pending or settled claims to report?
If you do not have any pending or settled claims, there is an option to check a box indicating this status. By doing so, you attest to the absence of such claims, which streamlines the application process. It is still important to sign the form to confirm this declaration.
How is the information from the form kept confidential?
The California Participating Practitioner form includes provisions that ensure the confidentiality of the information provided. The healthcare organization is committed to maintaining this information in a secure manner, sharing it only in the context of legitimate credentialing and peer review activities. Practitioners can feel assured that their personal and professional details will be handled with care and respect.
Completing the California Participating Practitioner form can be a straightforward process, but there are common mistakes that can lead to delays or complications. One frequent error is failing to provide complete information. Each section of the form must be filled out thoroughly. Incomplete answers can hinder the application process and may result in the need for additional follow-up or clarification.
Another mistake involves misunderstanding the requirement to report all professional liability lawsuits or arbitration actions. Some applicants mistakenly believe that only pending cases need to be disclosed. However, the form requires information on all cases from the past seven years, regardless of their current status. This oversight can lead to issues with compliance and may affect the applicant's credibility.
Additionally, applicants often overlook the importance of accurate case details. For instance, providing incorrect patient names, court case numbers, or dates can create confusion and may complicate the verification process. It is essential to double-check these details to ensure that they match official records.
Another common issue arises from not including the necessary supporting documentation. If the form requests additional narratives or clinical details, these should be attached as specified. Failing to include this information can result in a delay in processing the application.
Lastly, many applicants neglect to sign and date the form properly. The certification at the end of the document is crucial, as it attests to the truthfulness of the information provided. A missing signature or date can render the application invalid, leading to further delays in the review process.
The California Participating Practitioner form is a crucial document for healthcare professionals seeking participation in certain healthcare organizations. Several other forms and documents are often used alongside this application to ensure a comprehensive review of the practitioner's qualifications and history. Below is a list of related documents that may be required during the application process.
These documents collectively support the evaluation process for healthcare practitioners applying for participation in organizations. Ensuring all forms are completed accurately and submitted in a timely manner can facilitate a smoother application process.
When filling out the California Participating Practitioner form, there are important actions to take and pitfalls to avoid. Adhering to these guidelines can streamline the process and prevent delays.
Misconceptions about the California Participating Practitioner form can lead to confusion and errors in the application process. Here are ten common misconceptions, along with clarifications for each.
Understanding these misconceptions can help practitioners navigate the application process more effectively and ensure compliance with the requirements of the California Participating Practitioner form.
When filling out the California Participating Practitioner form, there are several important points to keep in mind. Here are key takeaways to ensure a smooth process:
Being thorough and accurate in completing the California Participating Practitioner form will help facilitate the evaluation of your application. It is important to provide truthful information and ensure that all necessary details are included.