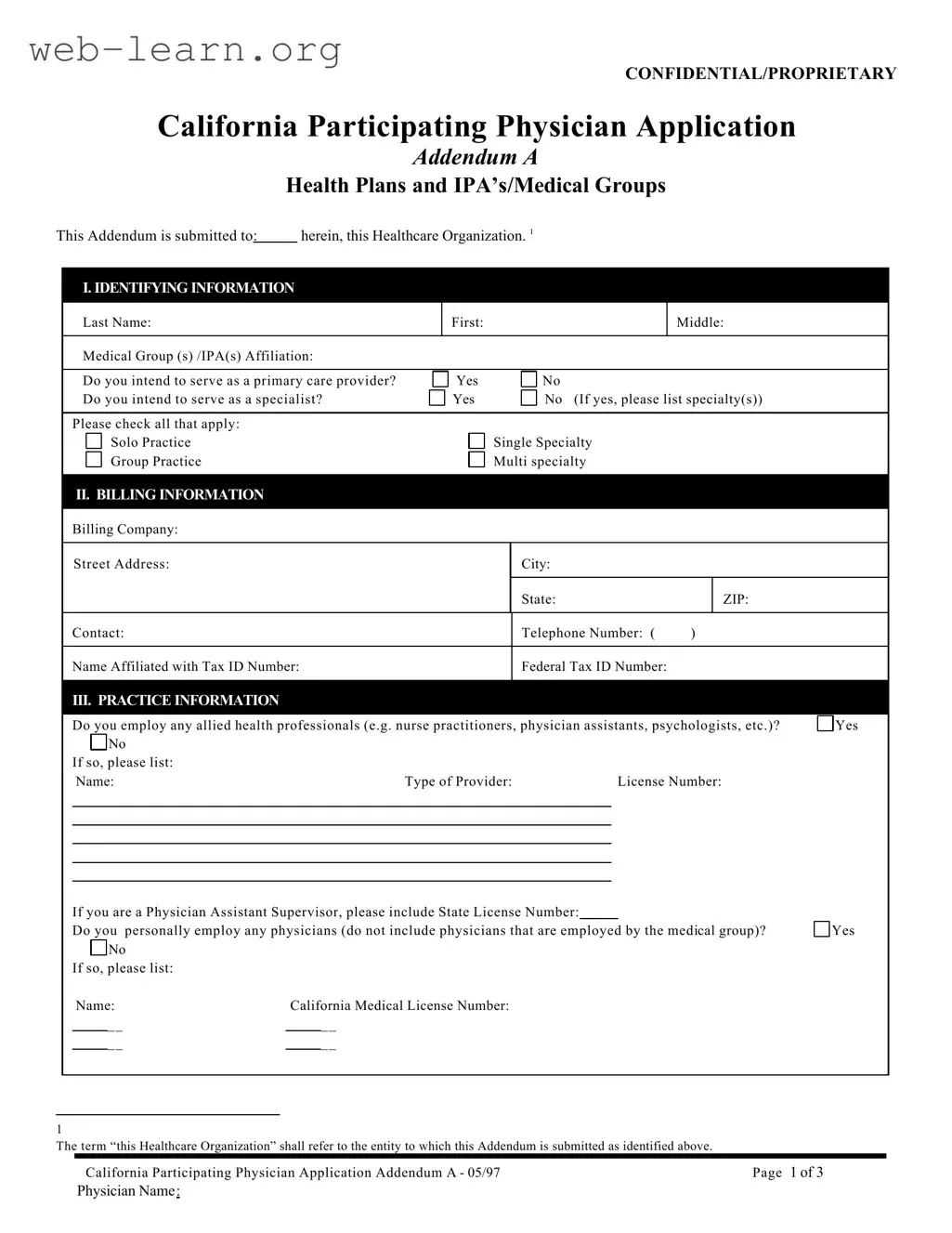
The California Participating Physician form serves as a vital document for healthcare professionals seeking to join various health plans and medical groups within the state. This comprehensive application captures essential identifying information, including the physician's name, medical group affiliations, and type of provider. It also addresses the physician's practice structure, whether they operate in solo or group settings, and whether they specialize in primary care or other specialties. The form delves into billing details, requiring the submission of the billing company information and tax identification numbers. Furthermore, it explores practice specifics, such as the employment of allied health professionals and the types of clinical services offered. Physicians are also prompted to disclose their office hours, coverage arrangements, and any relevant accreditations or certifications. Language proficiency and laboratory services are additional aspects covered, ensuring a holistic view of the physician's practice. This document ultimately facilitates a thorough evaluation of the physician's qualifications and capabilities, paving the way for their participation in California's healthcare landscape.

| Fact Name | Details |
|---|---|
| Governing Law | The California Participating Physician form is governed by California Business and Professions Code Section 2052. |
| Confidentiality | The form is marked as CONFIDENTIAL/PROPRIETARY, indicating that the information provided is sensitive and should be handled accordingly. |
| Primary Care Provider | Applicants must indicate whether they intend to serve as a primary care provider, which is a key aspect of their practice role. |
| Practice Information | Physicians are required to disclose if they employ allied health professionals, as this impacts the structure of their practice. |
| Accreditations | The form allows physicians to list any accreditations or certifications they have received, which can enhance their credibility. |
Completing the California Participating Physician form is essential for healthcare providers looking to participate in specific health plans or medical groups. This process involves gathering necessary information about your practice, affiliations, and professional qualifications. Following the steps outlined below will help ensure that you fill out the form accurately and completely.
What is the purpose of the California Participating Physician form?
The California Participating Physician form is designed to collect essential information from healthcare providers who wish to participate in specific health plans or medical groups. It ensures that the healthcare organization has the necessary details about the physician's qualifications, practice, and services offered.
What information is required on the form?
The form requires various types of information, including:
Who should complete the form?
Any physician who intends to participate in a health plan or medical group in California should complete this form. This includes primary care providers and specialists across various practice settings, whether solo or group practices.
Is the information submitted confidential?
Yes, the form is marked as confidential/proprietary, indicating that the information provided will be handled with care and is intended for use only by the healthcare organization to which it is submitted.
What should I do if I do not have hospital privileges?
If a physician does not have hospital privileges, the form requires the submission of a written plan for continuity of care. This plan should outline how the physician will ensure that patients receive ongoing care and support.
Are there any specific requirements for laboratory services?
Yes, if a physician provides direct laboratory services, they must include their Tax Identification Number (TIN) and Clinical Laboratory Information Act (CLIA) information. A copy of the CLIA certificate or waiver should also be attached if available.
What happens if the information provided is inaccurate?
Providing inaccurate information on the form can lead to complications in the physician's participation in health plans or medical groups. It is crucial that all details are accurate and up-to-date to avoid potential issues with credentialing or reimbursement.
How can I submit the completed form?
The completed form should be submitted to the designated healthcare organization or medical group as indicated on the form. Ensure that all required attachments are included and that the physician's signature is present, as stamped signatures are not acceptable.
Completing the California Participating Physician form can be a straightforward process, yet many applicants make common mistakes that can delay their application or lead to complications. Understanding these pitfalls can help ensure a smoother submission.
One frequent error is neglecting to provide complete identifying information. Applicants often forget to include their full names or license numbers. Missing this information can lead to confusion and may cause the application to be rejected. Ensuring that all personal details are accurately filled out is crucial for proper identification.
Another common mistake involves the billing information section. Applicants sometimes fail to provide the correct Tax Identification Number (TIN) or Federal Tax ID Number. This information is essential for processing payments and verifying the physician's business identity. Double-checking these numbers can prevent unnecessary delays.
Many applicants also overlook the practice information section. They may forget to indicate whether they employ allied health professionals or if they personally employ any physicians. Providing this information is vital, as it helps the healthcare organization understand the structure of the practice and the services offered.
Additionally, some physicians do not specify their clinical services accurately. Listing services that are not typically associated with their specialty or failing to mention those they do not perform can lead to misunderstandings about their capabilities. Clarity in this section is essential for ensuring appropriate patient referrals.
Another area where mistakes are common is in the office hours section. Applicants may either leave this section blank or provide incomplete information. Clearly indicating office hours helps patients and the healthcare organization know when the physician is available for consultations.
In the coverage of practice section, applicants sometimes forget to list their answering service and covering physicians. This information is crucial for ensuring continuity of care, especially when the primary physician is unavailable. Failing to provide this can compromise patient care.
Language proficiency is another area where errors can occur. Some applicants do not specify the foreign languages they or their staff speak fluently. This information is important for patient communication and can affect patient satisfaction and care quality.
Finally, applicants may overlook the professional organizations section. Listing relevant memberships can enhance a physician's credibility and demonstrate ongoing professional development. Neglecting to include this information can diminish the application’s overall strength.
By being aware of these common mistakes and taking the time to fill out the California Participating Physician form carefully, applicants can increase their chances of a successful application. Attention to detail is key in this process.
When completing the California Participating Physician form, several other documents may also be required or beneficial to ensure a smooth application process. Below is a list of commonly used forms and documents that accompany the California Participating Physician form.
Gathering these documents can help streamline the application process and facilitate quicker approval. Ensure that all information is accurate and up-to-date to avoid delays.
When filling out the California Participating Physician form, attention to detail is crucial. Here are seven things to keep in mind, including what to do and what to avoid:
Following these guidelines will help ensure a smooth application process and contribute to a successful partnership with healthcare organizations.
Misconceptions about the California Participating Physician form can lead to confusion among healthcare providers. Below are eight common misconceptions along with explanations to clarify them.
When filling out and using the California Participating Physician form, it is important to keep the following key takeaways in mind:
Completing the form accurately and thoroughly will help facilitate your participation in healthcare plans and ensure compliance with necessary regulations.