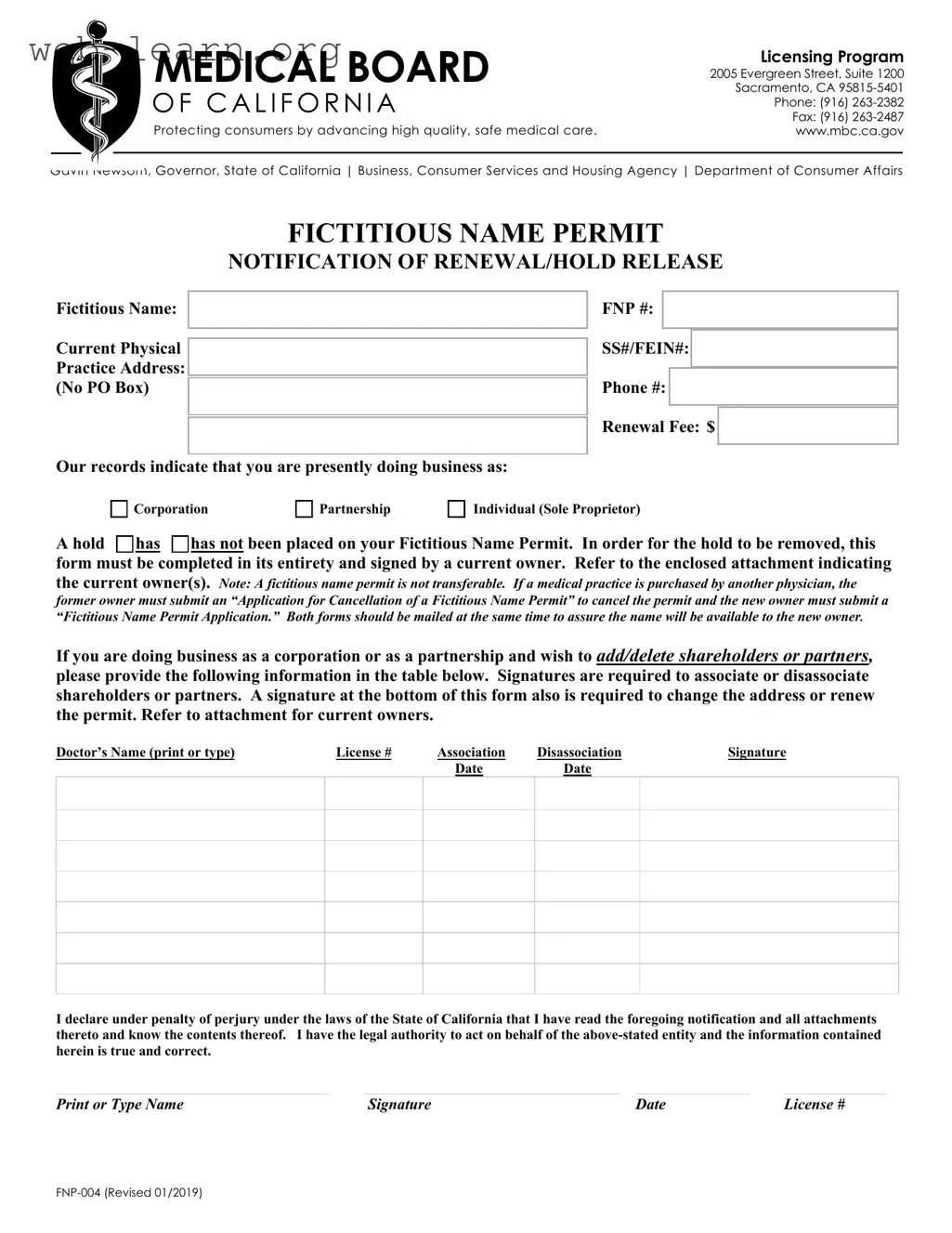
The California FNP 004 form plays a critical role in the management of fictitious name permits for medical practices. This form is essential for notifying the Medical Board of California about renewals or holds related to fictitious name permits. Practitioners must provide key information, including their fictitious name, physical practice address, and details about their business structure, whether it be a corporation, partnership, or sole proprietorship. The form also requires a renewal fee and includes a section for the current owners to sign, ensuring that all information is accurate and up-to-date. It is important to note that a fictitious name permit is not transferable; thus, if ownership of a medical practice changes, the previous owner must cancel the permit while the new owner submits a new application. Additionally, any changes in shareholders or partners must be documented through this form, highlighting the need for accurate record-keeping. The declaration at the end of the form affirms the legal authority of the signer, emphasizing the importance of compliance with California laws. Completing the FNP 004 form correctly is vital for maintaining the integrity and legality of medical practice operations in California.
| Fact Name | Details |
|---|---|
| Governing Law | The California FNP 004 form is governed by the Business and Professions Code, Section 17900 et seq. |
| Purpose | This form serves as a notification for the renewal or hold release of a fictitious name permit. |
| Fictitious Name | Users must provide their fictitious name and current physical practice address, which cannot be a P.O. Box. |
| Fees | A renewal fee of $X is required to process the form. (Note: The fee amount should be specified.) |
| Ownership Changes | The form must be signed by a current owner to remove any holds on the fictitious name permit. |
| Transferability | A fictitious name permit is not transferable; a new application is needed if the practice is sold. |
| Legal Declaration | Signatories must declare under penalty of perjury that the information provided is accurate and complete. |
Completing the California FNP 004 form is an essential step for those looking to manage their fictitious name permit effectively. This process ensures that all necessary information is accurately recorded and that the permit remains valid. Follow the steps outlined below to fill out the form correctly.
What is the purpose of the California FNP 004 form?
The California FNP 004 form is primarily used for the notification of renewal or hold release for a fictitious name permit. This permit allows healthcare providers to operate under a name that is different from their legal business name. It ensures that the public is aware of who is providing medical services, thereby promoting transparency and trust in healthcare practices.
Who needs to fill out the FNP 004 form?
Any individual or entity currently holding a fictitious name permit in California must complete the FNP 004 form when renewing their permit or if they need to release a hold on it. This includes corporations, partnerships, and sole proprietors. If there are changes in ownership, such as adding or removing partners or shareholders, the form must also be filled out to reflect these changes.
What information is required on the form?
When completing the FNP 004 form, you will need to provide several key pieces of information:
Additionally, if there are any changes in ownership, you must include the names and signatures of current owners, as well as details regarding any new partners or shareholders.
What happens if I do not submit the FNP 004 form?
Failing to submit the FNP 004 form on time can result in a hold being placed on your fictitious name permit. This can prevent you from legally operating under your chosen fictitious name. It is crucial to complete and submit the form in its entirety to avoid any disruptions in your practice. If your permit is canceled or on hold, you may need to go through a more complicated process to reinstate it.
Filling out the California FNP 004 form can be straightforward, but common mistakes can lead to delays or complications. One frequent error is failing to provide a complete physical practice address. The form explicitly states that a PO Box is not acceptable. This omission can result in processing delays, as the Medical Board requires a valid physical address to maintain accurate records.
Another common mistake involves the incorrect identification of the business structure. Applicants often misclassify their practice as a corporation, partnership, or sole proprietorship. It is essential to select the appropriate category, as each has different legal implications and requirements. Misclassification can lead to unnecessary complications, especially if the business structure changes in the future.
Additionally, signatures play a critical role in the completion of the form. Many applicants neglect to ensure that all required signatures are present. This includes signatures for both associating and disassociating shareholders or partners, as well as the final declaration at the bottom of the form. A missing signature can halt the processing of the application and necessitate resubmission.
Lastly, applicants often overlook the importance of accuracy in the information provided. Mistakes in the FNP number, Social Security number, or Federal Employer Identification Number can cause significant delays. It is crucial to double-check all entries for accuracy before submission. Taking the time to review the form can prevent unnecessary setbacks and ensure a smoother renewal process.
The California FNP 004 form, which is used for Fictitious Name Permit Notification of Renewal or Hold Release, is often accompanied by several other important documents. Each of these forms plays a crucial role in ensuring compliance with state regulations and maintaining accurate records for medical practices. Below is a list of documents that are commonly used alongside the FNP 004 form.
These forms and documents are essential for maintaining compliance and ensuring the smooth operation of medical practices in California. Each serves a specific purpose and contributes to the overall integrity of the healthcare system.
When filling out the California FNP 004 form, it is essential to approach the task with care and attention to detail. Below is a list of important dos and don'ts to guide you through the process.
By adhering to these guidelines, you can help ensure a smoother and more efficient process in managing your fictitious name permit. Your attention to detail is crucial in maintaining compliance with California regulations.
There are several misconceptions about the California FNP 004 form that can lead to confusion. Understanding these can help ensure compliance and smooth processing. Here are five common misconceptions:
This form is applicable to various business structures, including partnerships and sole proprietors. All entities doing business under a fictitious name must complete it.
This is incorrect. A fictitious name permit is not transferable. When ownership changes, the former owner must cancel the permit, and the new owner must apply for a new permit.
In cases of adding or removing shareholders or partners, signatures from all relevant parties are required. This ensures that all changes are officially recognized.
Completing the form fully is essential. Incomplete forms may lead to delays or rejection of the application, which can hinder business operations.
This is a critical error. Any changes to the business address must be reported using the FNP 004 form to keep records accurate and up to date.
When filling out and using the California FNP 004 form, keep these key takeaways in mind: