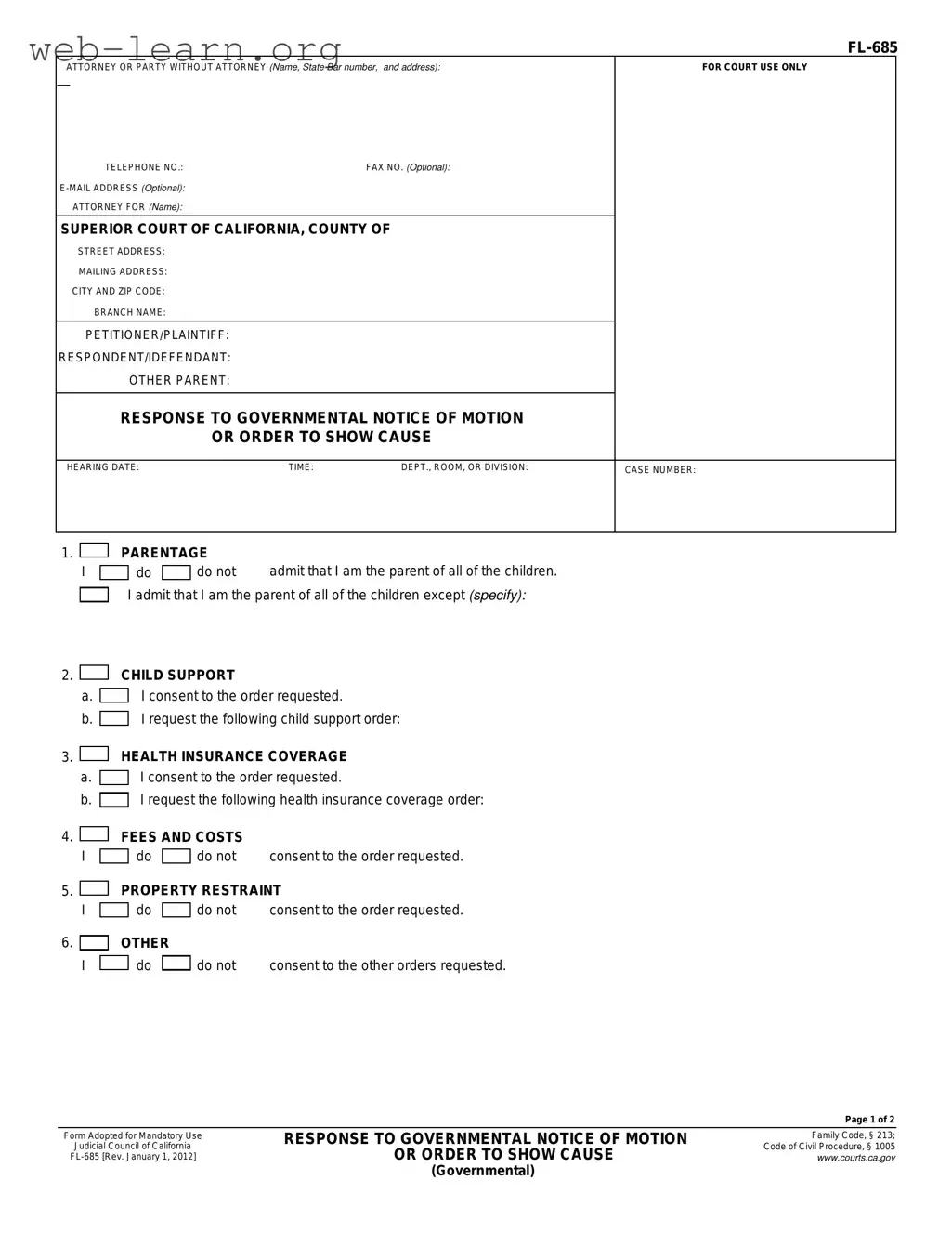
The California FL-685 form plays a crucial role in family law proceedings, particularly in cases involving child support and parental responsibilities. This form is designed for individuals responding to a governmental notice of motion or order to show cause, which may arise during legal disputes concerning child custody, visitation, or support. By completing the FL-685, a respondent can address several important issues, such as admitting or denying parentage of the children involved, consenting to proposed child support or health insurance orders, and responding to other related requests from the court. Additionally, the form requires the respondent to provide facts in support of their response, which may be detailed in an attached declaration. It is important to note that the form also includes sections for proof of service, ensuring that all parties involved are properly notified of the proceedings. The FL-685 must be completed accurately and submitted in a timely manner to uphold the legal rights of the parties involved and to facilitate the court's decision-making process.
| Fact Name | Details |
|---|---|
| Purpose | The FL-685 form is used to respond to a governmental notice of motion or order to show cause regarding parentage and child support issues. |
| Governing Laws | This form is governed by California Family Code, § 213 and the Judicial Council of California Code of Civil Procedure, § 1005. |
| Signature Requirement | The form must be signed by the declarant, confirming that the information provided is true under penalty of perjury. |
| Proof of Service | A proof of service section is included, which outlines how the response should be mailed to the involved parties. |
Filling out the California FL-685 form is an important step in responding to a governmental notice regarding child support or other related matters. This form allows you to present your position clearly and concisely to the court. Ensuring that all information is accurate and complete will help facilitate the process.
Once you have filled out the form completely, make sure to keep a copy for your records. Then, submit the form to the court and serve copies to the other parties involved. Following these steps diligently will ensure that your response is properly filed and considered by the court.
The California FL 685 form serves as a response to a governmental notice of motion or order to show cause. It is used in family law cases to address issues such as parentage, child support, health insurance coverage, and other related orders. This form allows individuals to formally state their position regarding these matters in court.
The FL 685 form is intended for individuals involved in family law proceedings where a governmental agency has initiated a motion or order. This includes parents or guardians who need to respond to issues concerning child support, custody, or visitation rights. It is important for the responding party to complete this form accurately to ensure their voice is heard in the legal process.
When completing the FL 685 form, you will need to provide the following information:
After completing the FL 685 form, it must be filed with the appropriate Superior Court in California. It is essential to ensure that the form is submitted by the deadline specified in the governmental notice. Additionally, you must serve a copy of the completed form to all other parties involved in the case, which can be done via mail or in person.
Once the FL 685 form is submitted and served, the court will review the responses provided. A hearing may be scheduled where all parties can present their arguments. The court will then make a decision based on the evidence and information presented, which may include orders related to child support, custody, and other matters.
If circumstances change or if you need to clarify your response, it is possible to amend your submission. You may need to file an amended FL 685 form with the court and serve it to all involved parties. It is advisable to consult with a legal professional to ensure that the amendment is done correctly and in accordance with court rules.
For more information about the FL 685 form and family law procedures, you can visit the California Courts website. Local family law facilitators and legal aid organizations can also provide assistance. They can help clarify any questions you may have and guide you through the process.
When filling out the California FL-685 form, people often make several common mistakes that can lead to complications in their case. One frequent error is failing to clearly specify the names of all children involved. This form requires individuals to admit parentage for each child, and omitting a child's name can create confusion or delays in processing.
Another mistake is neglecting to provide accurate contact information. The form asks for the attorney's or party's name, address, and phone number. If this information is incorrect or incomplete, it may hinder communication regarding the case.
Many individuals also forget to sign the form. A signature is necessary to validate the information provided. Without it, the court may reject the submission, requiring the individual to start over.
Some people mistakenly think they can skip sections they feel are not applicable to their situation. Each part of the form should be addressed, even if the answer is "do not consent." Leaving sections blank can lead to misunderstandings or assumptions by the court.
Misunderstanding the consent options is another common issue. Individuals may accidentally indicate consent to orders they do not agree with. It is crucial to carefully read each option and select the correct response.
Additionally, failing to attach necessary supporting documents can be problematic. The form may require declarations or other evidence to support the claims made. Not including these documents can delay the process.
People often overlook the proof of service section as well. This part confirms that the response has been properly served to all parties involved. Without this proof, the court may not recognize that all parties were notified.
Another mistake is not keeping a copy of the completed form for personal records. Having a copy can be helpful for future reference and ensures that individuals have a record of what was submitted.
Lastly, individuals may forget to check for any updates or changes to the form itself. Legal forms can be revised, and using an outdated version may lead to complications. Always verify that the most current version is being used.
The California FL-685 form is an essential document used in family law cases, particularly those involving child support and parental rights. Alongside this form, several other documents may be required to provide additional context or fulfill legal requirements. Below is a list of other forms and documents commonly associated with the FL-685 form.
Understanding these forms and their purposes can help individuals navigate the complexities of family law in California. Each document plays a significant role in ensuring that the rights of all parties, especially children, are protected throughout the legal process.
When filling out the California FL-685 form, it's essential to approach the process with care. Here are ten things to keep in mind, including what to do and what to avoid.
By following these guidelines, you can navigate the completion of the FL-685 form more effectively. Taking the time to do it right can help avoid complications down the line.
Misconceptions about the California FL-685 form can lead to confusion and mistakes. Here are four common misunderstandings:
Understanding these points can help individuals navigate the legal process more effectively.
Filling out and using the California FL-685 form can be a straightforward process if you keep in mind a few key points. Here are some essential takeaways:
By keeping these points in mind, you can navigate the FL-685 form with greater confidence and clarity.